

Arterial stiffening is a crucial factor for left ventricular diastolic dysfunction in a community-based normotensive population
- PMID: 33447764
- PMCID: PMC7803042
- DOI: 10.1016/j.ijchy.2020.100038
Arterial stiffening is a crucial factor for left ventricular diastolic dysfunction in a community-based normotensive population
Abstract
Background: Left ventricular (LV) diastolic dysfunction is an important underlying hemodynamic mechanism for heart failure. Hypertension reportedly increases aortic stiffness with histological changes in the aorta assessed using aortic pulse wave velocity (PWV) that is associated with LV diastolic dysfunction. The role of hypertension per se in the relationship between aortic stiffness and LV diastolic dysfunction has not been clarified; therefore, we investigated whether this relation works for normotensive subjects.
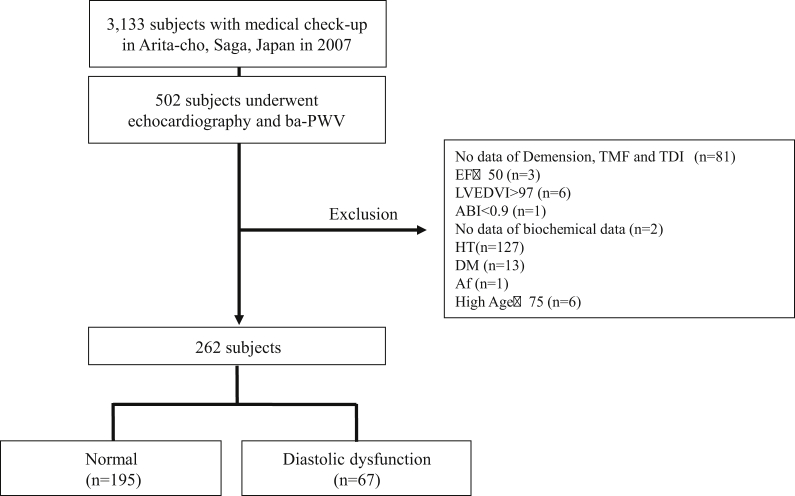
Methods: Of the 502 subjects who underwent both echocardiography and PWV measurement in a medical check-up conducted in Arita, Japan, we enrolled 262 consecutive normotensive subjects (age 52 ± 13 years). LV diastolic dysfunction was defined as abnormal relaxation and pseudonormal or restrictive patterns determined with both transmitral flow velocity and mitral annular velocity. Aortic stiffness was assessed via non-invasive brachial-ankle PWV measurement.
Results: LV diastolic dysfunction was detected in 67 of the 262 (26%) normotensive subjects, and PWV was higher in subjects with LV diastolic dysfunction (15.4 ± 3.6 vs. 13.0 ± 2.7 m/s, p < 0.01). Multivariate logistic regression analyses revealed that PWV was independently associated with LV diastolic dysfunction (p = 0.02) after the adjustment for age; body mass index; blood pressure; eGFR; blood levels of BNP, glucose, and HDL cholesterol; LV mass index; and LA dimension.
Conclusions: Both aortic stiffness and LV diastolic function are mutually related even in normotensive subjects, independent of the potential confounding factors. The increase in aortic stiffness may be a risk factor for LV diastolic dysfunction, irrespective of blood pressure.
Keywords: Diastolic function; Normotension; Pulse wave velocity.
© 2020 The Authors.
Conflict of interest statement
All co-authors of this manuscript have read and approved the submission of the manuscript. All of the authors have made an important contribution to the study and are thoroughly familiar with the original data. All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest: Dr. Maeda have nothing to disclose; Dr. Kanzaki have nothing to disclose; Dr. Hasegawa reports other from Takeda Pharmaceutical Company Limited, other from Daiichi-Sankyo Company, Limited, other from Otsuka Pharmaceutical Co., Ltd., other from Bayer Yakuhin, Ltd, other from Mitsubishi Tanabe Pharma Corporation, other from Abbott Vascular Japan Co., Ltd., other from Shionogi & Co., Ltd.; Dr. Fukuda and Kim reports have nothing to disclose; Dr. Asakura reports grants from Acterion Pharmaceutical Japan, grants from Boehringer Ingelheim Japan, Inc., personal fees from Otsuka Pharmaceutical Co., Ltd., personal fees from Sanofi K·K., personal fees from Bayer Yakuhin, Ltd., personal fees from MSD K·K., personal fees from Takeda Pharmaceutical Company Limited., personal fees from Ono, personal fees from Mitsubishi Tanabe Pharma Corporation, personal fees from Daiichi-sankyo, personal fees from Pfizer Japan Inc., personal fees from Astellas Amgen Biopharma, outside the submitted work; Dr. Asanuma reports have nothing to disclose; Dr. Amaki reports grants from Japan Heart Foundation/Bayer Yakuhin Research Grant Abroad, grants from Suzuken Memorial Foundation, non-financial support from Abbott Vascular Japan, non-financial support from Takeda Pharmaceutical Company, outside the submitted work; Dr. Nishimura reports have nothing to disclose; Dr. Kitakaze reports grants and personal fees from Takeda, during the conduct of the study; grants from Japanese government, grants from Japan Heart Foundation, grants from Japan Cardiovascular Research Foundation, grants and personal fees from Asteras, grants and personal fees from Sanofi, personal fees from Daiichi-sankyo, grants and personal fees from Pfizer, grants and personal fees from Ono, personal fees from Bayer, grants and personal fees from Novartis, personal fees from Bheringer, grants and personal fees from Tanabe-mitubishi, personal fees from Kowa, grants and personal fees from Kyowa-hakko-kirin, personal fees from Dainihon-sumitomo, personal fees from Sawai, personal fees from MSD, grants and personal fees from Abott, grants and personal fees from Otsuka, grants from Calpis, grants from Nihon Kohden, personal fees from Shionogi, personal fees from Astrazeneca, personal fees from Asahikasei Med., personal fees from Novo nordisk, personal fees from Fuji-film RI, personal fees from Japan Medical Data, outside the submitted work.
Figures
References
-
- Nichols W.W., O'Rourke M.F. 3rd ed. 2005. McDonald's Blood Flow in Arteries; pp. 12–71. Philadelphia, PA, USA(Reference to a chapter in an edited book:)
-
- Safar M., An O.R.M.E. 1st ed. vol. 23. Elsevier; 2006. pp. 225–256. (Arterial Stiffness in Hypertension). (Reference to a chapter in an edited book:)
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
