

C-reactive protein and clinical outcomes in patients with COVID-19
- PMID: 33448289
- PMCID: PMC7928982
- DOI: 10.1093/eurheartj/ehaa1103
C-reactive protein and clinical outcomes in patients with COVID-19
Abstract
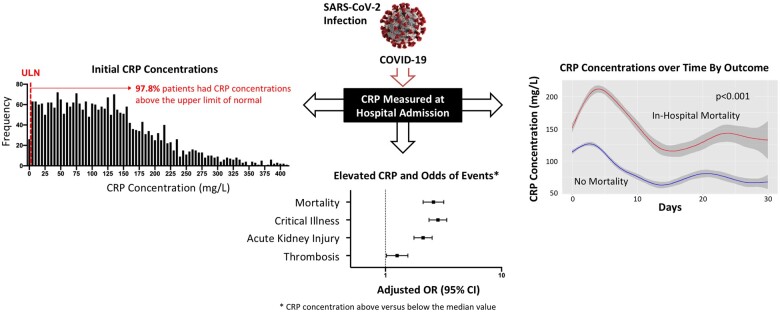
Background: A systemic inflammatory response is observed in coronavirus disease 2019 (COVID-19). Elevated serum levels of C-reactive protein (CRP), a marker of systemic inflammation, are associated with severe disease in bacterial or viral infections. We aimed to explore associations between CRP concentration at initial hospital presentation and clinical outcomes in patients with COVID-19.
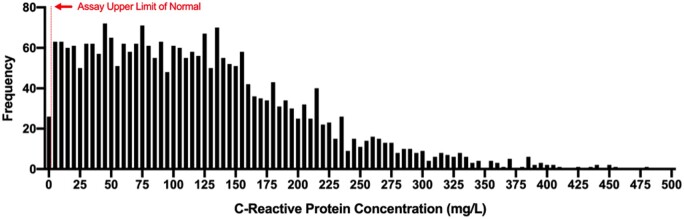
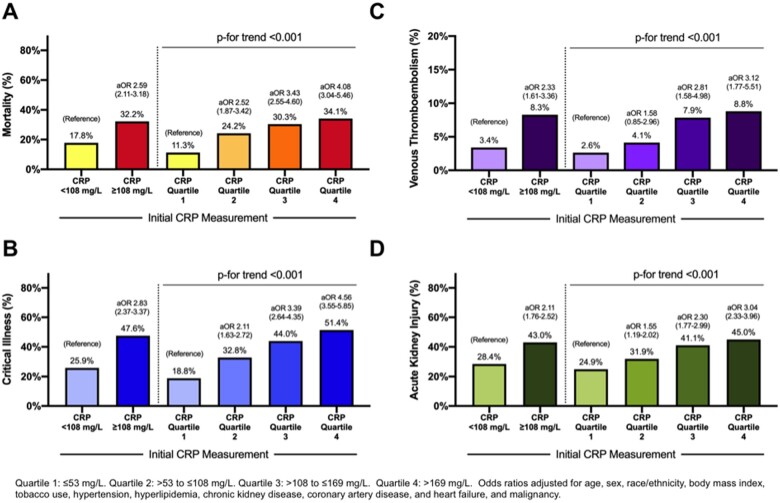
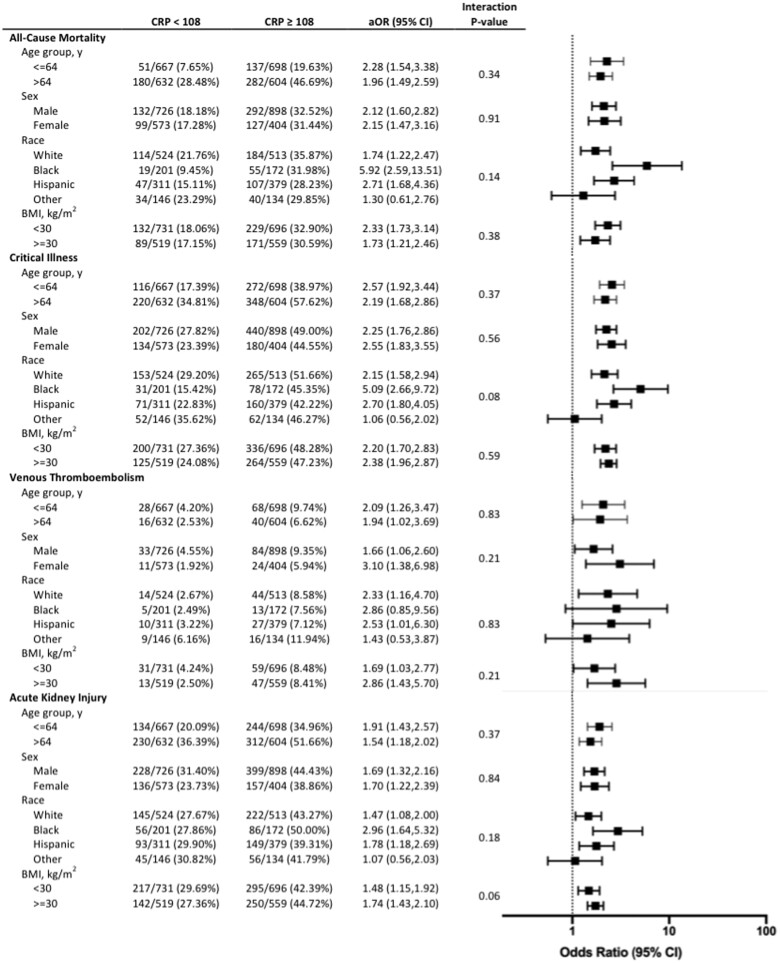
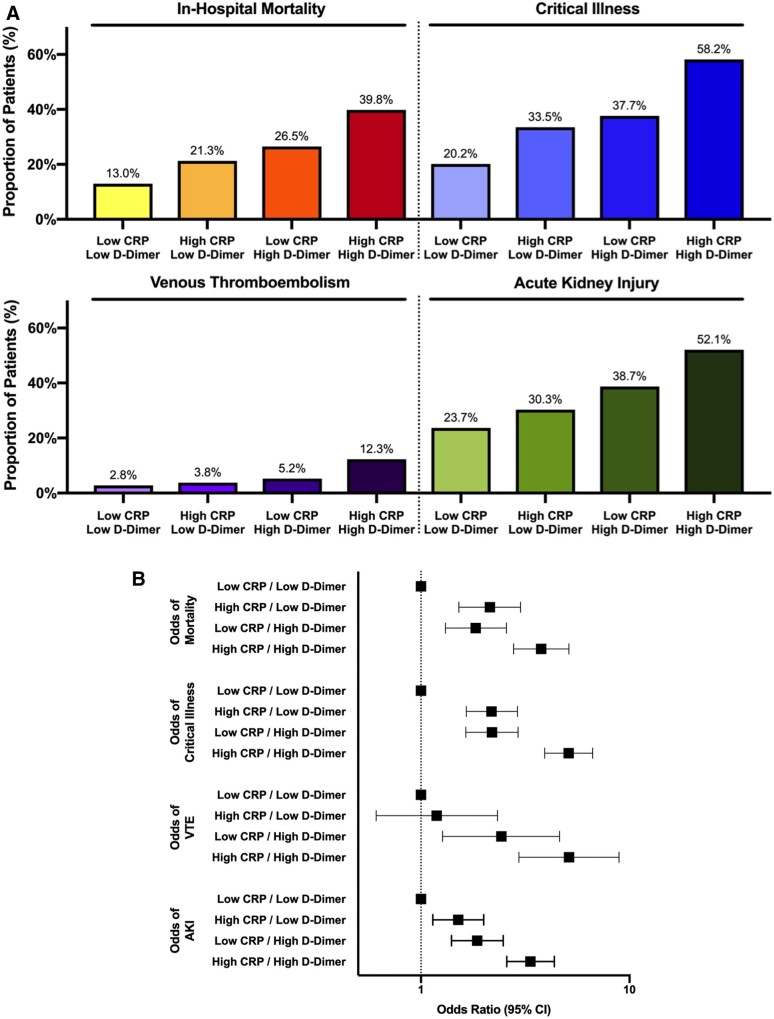
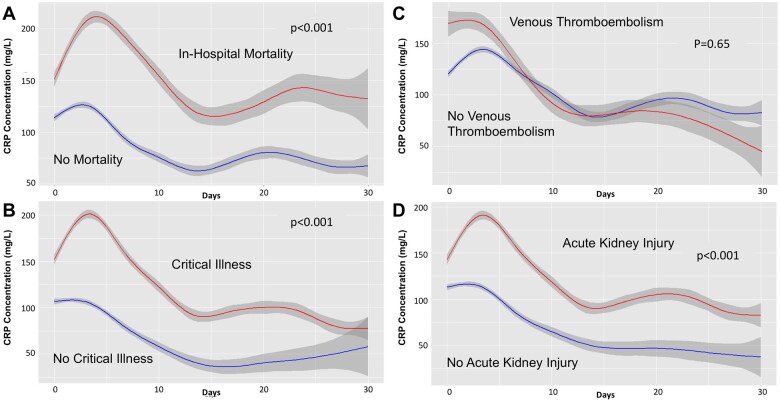
Methods and results: Consecutive adults aged ≥18 years with COVID-19 admitted to a large New York healthcare system between 1 March and 8 April 2020 were identified. Patients with measurement of CRP were included. Venous thrombo-embolism (VTE), acute kidney injury (AKI), critical illness, and in-hospital mortality were determined for all patients. Among 2782 patients hospitalized with COVID-19, 2601 (93.5%) had a CRP measurement [median 108 mg/L, interquartile range (IQR) 53-169]. CRP concentrations above the median value were associated with VTE [8.3% vs. 3.4%; adjusted odds ratio (aOR) 2.33, 95% confidence interval (CI) 1.61-3.36], AKI (43.0% vs. 28.4%; aOR 2.11, 95% CI 1.76-2.52), critical illness (47.6% vs. 25.9%; aOR 2.83, 95% CI 2.37-3.37), and mortality (32.2% vs. 17.8%; aOR 2.59, 95% CI 2.11-3.18), compared with CRP below the median. A dose response was observed between CRP concentration and adverse outcomes. While the associations between CRP and adverse outcomes were consistent among patients with low and high D-dimer levels, patients with high D-dimer and high CRP have the greatest risk of adverse outcomes.
Conclusions: Systemic inflammation, as measured by CRP, is strongly associated with VTE, AKI, critical illness, and mortality in COVID-19. CRP-based approaches to risk stratification and treatment should be tested.
Keywords: C-reactive protein; COVID-19; Coronavirus; Critical illness; Inflammation; Mortality.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2021. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
C-reactive protein predicts outcome in COVID-19: is it also a therapeutic target?Eur Heart J. 2021 Jun 14;42(23):2280-2283. doi: 10.1093/eurheartj/ehab169. Eur Heart J. 2021. PMID: 33778886 Free PMC article. No abstract available.
References
-
- Petrilli CM, Jones SA, Yang J, Rajagopalan H, O’Donnell L, Chernyak Y, Tobin KA, Cerfolio RJ, Francois F, Horwitz LI. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study. BMJ 2020;369 : m1966. - PMC - PubMed
-
- Morley JJ, Kushner I. Serum C-reactive protein levels in disease. Ann N Y Acad Sci 1982;389:406–418. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
