

The Effect of Psychiatric Comorbidities on Headache-Related Disability in Migraine: Results From the Chronic Migraine Epidemiology and Outcomes (CaMEO) Study
- PMID: 33448374
- PMCID: PMC7496280
- DOI: 10.1111/head.13914
The Effect of Psychiatric Comorbidities on Headache-Related Disability in Migraine: Results From the Chronic Migraine Epidemiology and Outcomes (CaMEO) Study
Abstract
Objective: To examine the influences of depression and anxiety on headache-related disability in people with episodic migraine or chronic migraine.
Background: Depression and anxiety are common comorbidities in people with migraine, especially among those with chronic migraine.
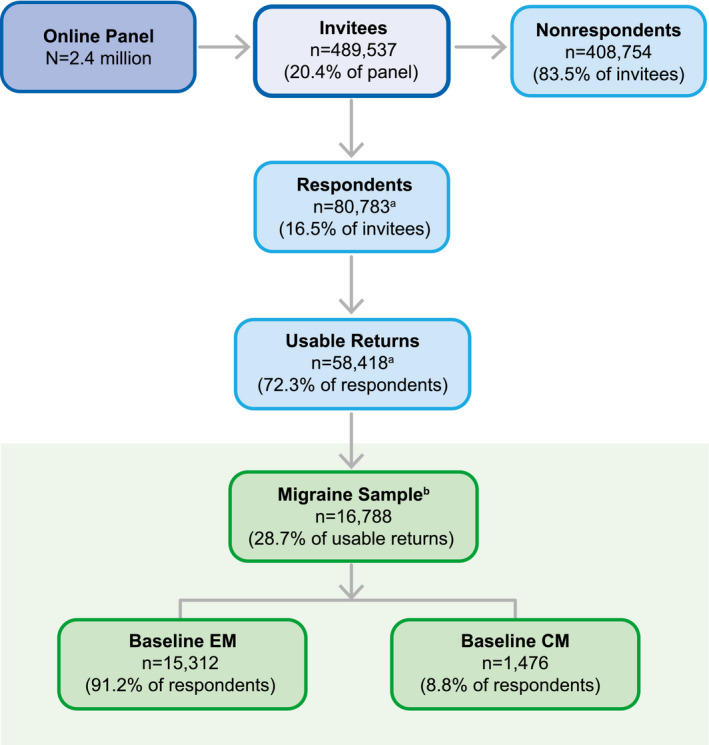
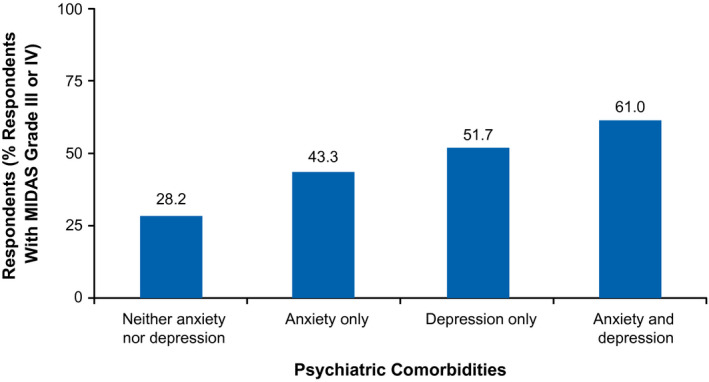
Methods: This cross-sectional analysis of data from the longitudinal, internet-based Chronic Migraine Epidemiology and Outcomes Study assessed sociodemographic and headache features, and headache-related disability (Migraine Disability Assessment Scale). Four groups were defined based on scores from validated screeners for depression (9-item Patient Health Questionnaire) and anxiety (7-item Generalized Anxiety Disorder Scale): depression alone, anxiety alone, both, or neither.
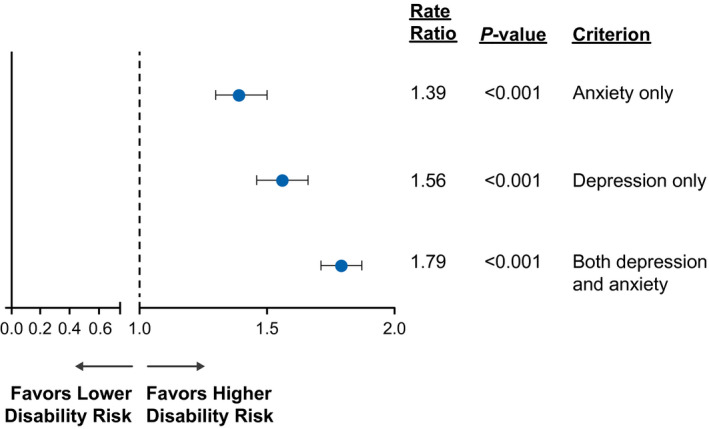
Results: Respondents (N = 16,788) were predominantly women (74.4% [12,494/16,788]) and white (84.0% [14,044/16,788]); mean age was 41 years. Depression was more likely in persons with chronic migraine vs episodic migraine (56.6% [836/1476] vs 30.0% [4589/15,312]; P < .001), as were anxiety (48.4% [715/1476] vs 28.1% 4307/15,312]; P < .001) and coexisting depression and anxiety (42.0% [620/1476] vs 20.8% [3192/15,312]; P < .001). After controlling for headache frequency and other covariates, depression alone, and anxiety alone were associated with 56.0% (rate ratio [RR], 1.56; 95% confidence interval [CI], 1.46-1.66) and 39.0% (RR, 1.39; 95% CI, 1.30-1.50) increased risks of moderate/severe migraine-related disability (both P < .001), respectively; the combination had an even greater effect on risk of moderate/severe disability (79.0% increase; RR, 1.79; 95% CI, 1.71-1.87; P < .001).
Conclusions: Depression alone and anxiety alone are associated with greater headache-related disability after controlling for sociodemographic and headache features. Coexisting depression and anxiety are more strongly associated with disability than either comorbidity in isolation. Interventions targeting depression and anxiety as well as migraine itself may improve headache-related disability in people with migraine.
Keywords: anxiety; comorbidity; depression; headache‐related disability; migraine.
© 2020 The Authors. Headache: The Journal of Head and Face Pain published by Wiley Periodicals LLC on behalf of American Headache Society.
Figures

References
-
- Headache Classification Committee of the International Headache Society . The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38:1‐211. - PubMed
-
- Pietrobon D, Moskowitz MA. Pathophysiology of migraine. Annu Rev Physiol. 2013;75:365‐391. - PubMed
-
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators . Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990‐2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1211‐1259. - PMC - PubMed
-
- Hamelsky SW, Lipton RB. Psychiatric comorbidity of migraine. Headache. 2006;46:1327‐1333. - PubMed
-
- Seng EK, Seng CD. Understanding migraine and psychiatric comorbidity. Curr Opin Neurol. 2016;29:309‐313. - PubMed
