

Accuracy of Magnetic Resonance Imaging-Guided Biopsy to Verify Breast Cancer Pathologic Complete Response After Neoadjuvant Chemotherapy: A Nonrandomized Controlled Trial
- PMID: 33449096
- PMCID: PMC7811182
- DOI: 10.1001/jamanetworkopen.2020.34045
Accuracy of Magnetic Resonance Imaging-Guided Biopsy to Verify Breast Cancer Pathologic Complete Response After Neoadjuvant Chemotherapy: A Nonrandomized Controlled Trial
Abstract
Importance: After neoadjuvant chemotherapy (NAC), pathologic complete response (pCR) is an optimal outcome and a surrogate end point for improved disease-free and overall survival. To date, surgical resection remains the only reliable method for diagnosing pCR.
Objective: To evaluate the accuracy of magnetic resonance imaging (MRI)-guided biopsy for diagnosing a pCR after NAC compared with reference-standard surgical resection.
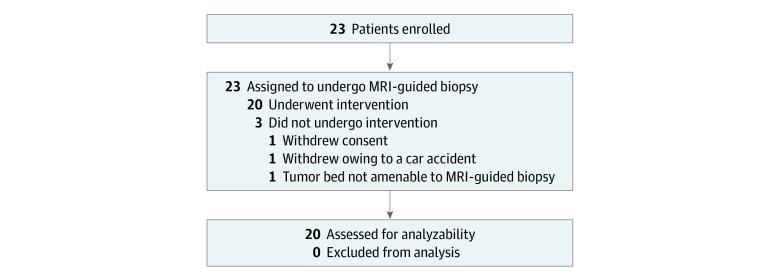
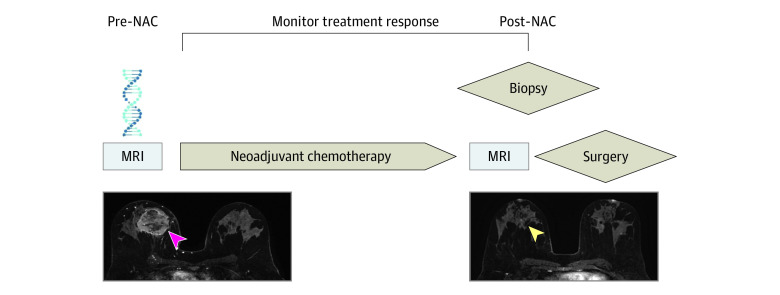
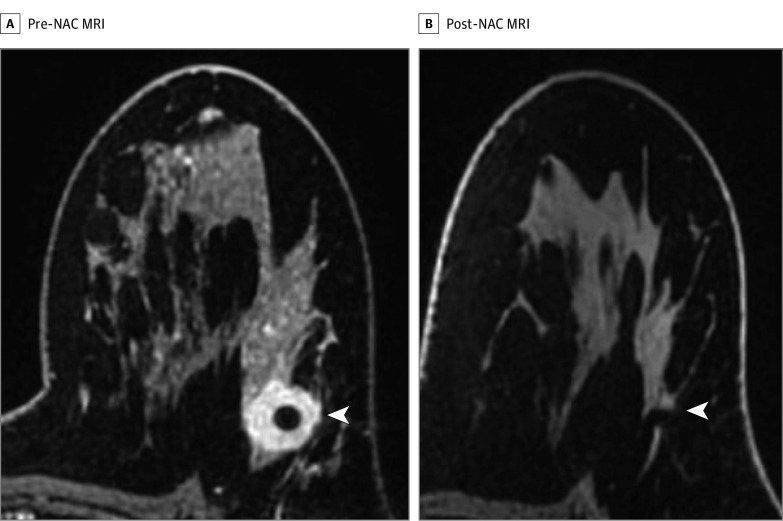
Design, setting, and participants: Single-arm, phase 1, nonrandomized controlled trial in a single tertiary care cancer center from September 26, 2017, to July 29, 2019. The median follow-up was 1.26 years (interquartile range, 0.85-1.59 years). Data analysis was performed in November 2019. Eligible patients had (1) stage IA to IIIC biopsy-proven operable invasive breast cancer; (2) standard-of-care NAC; (3) MRI before and after NAC, with imaging complete response defined as no residual enhancement on post-NAC MRI; and (4) definitive surgery. Patients were excluded if they were younger than 18 years, had a medical reason precluding study participation, or had a prior history of breast cancer.
Interventions: Post-NAC MRI-guided biopsy without the use of intravenous contrast of the tumor bed before definitive surgery.
Main outcomes and measures: The primary end point was the negative predictive value of MRI-guided biopsy, with true-negative defined as negative results of the biopsy (ie, no residual cancer) corresponding to a surgical pCR. Accuracy, sensitivity, positive predictive value, and specificity were also calculated. Two clinical definitions of pCR were independently evaluated: definition 1 was no residual invasive cancer; definition 2, no residual invasive or in situ cancer.
Results: Twenty of 23 patients (87%) had evaluable data (median [interquartile range] age, 51.5 [39.0-57.5] years; 20 women [100%]; 13 White patients [65%]). Of the 20 patients, pre-NAC median tumor size on MRI was 3.0 cm (interquartile range, 2.0-5.0 cm). Nineteen of 20 patients (95%) had invasive ductal carcinoma; 15 of 20 (75%) had stage II cancer; 11 of 20 (55%) had ERBB2 (formerly HER2 or HER2/neu)-positive cancer; and 6 of 20 (30%) had triple-negative cancer. Surgical pathology demonstrated a pCR in 13 of 20 (65%) patients and no pCR in 7 of 20 patients (35%) when pCR definition 1 was used. Results of MRI-guided biopsy had a negative predictive value of 92.8% (95% CI, 66.2%-99.8%), with accuracy of 95% (95% CI, 75.1%-99.9%), sensitivity of 85.8% (95% CI, 42.0%-99.6%), positive predictive value of 100%, and specificity of 100% for pCR definition 1. Only 1 patient had a false-negative MRI-guided biopsy result (surgical pathology showed <0.02 cm of residual invasive cancer).
Conclusions and relevance: This study's results suggest that the accuracy of MRI-guided biopsy to diagnose a post-NAC pCR approaches that of reference-standard surgical resection. MRI-guided biopsy may be a viable alternative to surgical resection for this population after NAC, which supports the need for further investigation.
Trial registration: ClinicalTrials.gov Identifier: NCT03289195.
Conflict of interest statement
Figures
References
-
- Boughey JC, McCall LM, Ballman KV, et al. Tumor biology correlates with rates of breast-conserving surgery and pathologic complete response after neoadjuvant chemotherapy for breast cancer: findings from the ACOSOG Z1071 (Alliance) Prospective Multicenter Clinical Trial. Ann Surg. 2014;260(4):608-614. doi: 10.1097/SLA.0000000000000924 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
