

Facility-Level Variation in Dialysis Use and Mortality Among Older Veterans With Incident Kidney Failure
- PMID: 33449098
- PMCID: PMC7811178
- DOI: 10.1001/jamanetworkopen.2020.34084
Facility-Level Variation in Dialysis Use and Mortality Among Older Veterans With Incident Kidney Failure
Abstract
Importance: Current guidelines lack consensus regarding the treatment of patients who may not benefit from dialysis; this lack of consensus may be associated with the substantial variation in dialysis use and outcomes across health care facilities.
Objective: To assess the degree to which variation in dialysis use and mortality was associated with patient rather than facility characteristics and to distinguish which features identified the US Department of Veterans Affairs (VA) facilities with high rates of dialysis use.
Design, setting, and participants: This cohort study analyzed data of veterans with stage 3 or 4 chronic kidney disease that progressed to kidney failure between January 1, 2011, and December 31, 2014. These patients received care from VA facilities across the US. Data sources included laboratory and administrative records from the VA, Medicare, and United States Renal Data System. Data analysis was conducted from August 1, 2019, to September 1, 2020.
Exposures: The primary exposure was the VA facility in which patients received most of their care before the onset of incident kidney failure defined as the first occurrence of either a sustained estimated glomerular filtration rate of less than 15 mL/min/1.73 m2 or the initiation of maintenance dialysis.
Main outcomes and measures: The primary outcomes were dialysis use and mortality within 2 years of incident kidney failure. Median rate ratio was used to quantify facility-level variation, and variance partition coefficient was used to quantify the sources of unexplained variation.
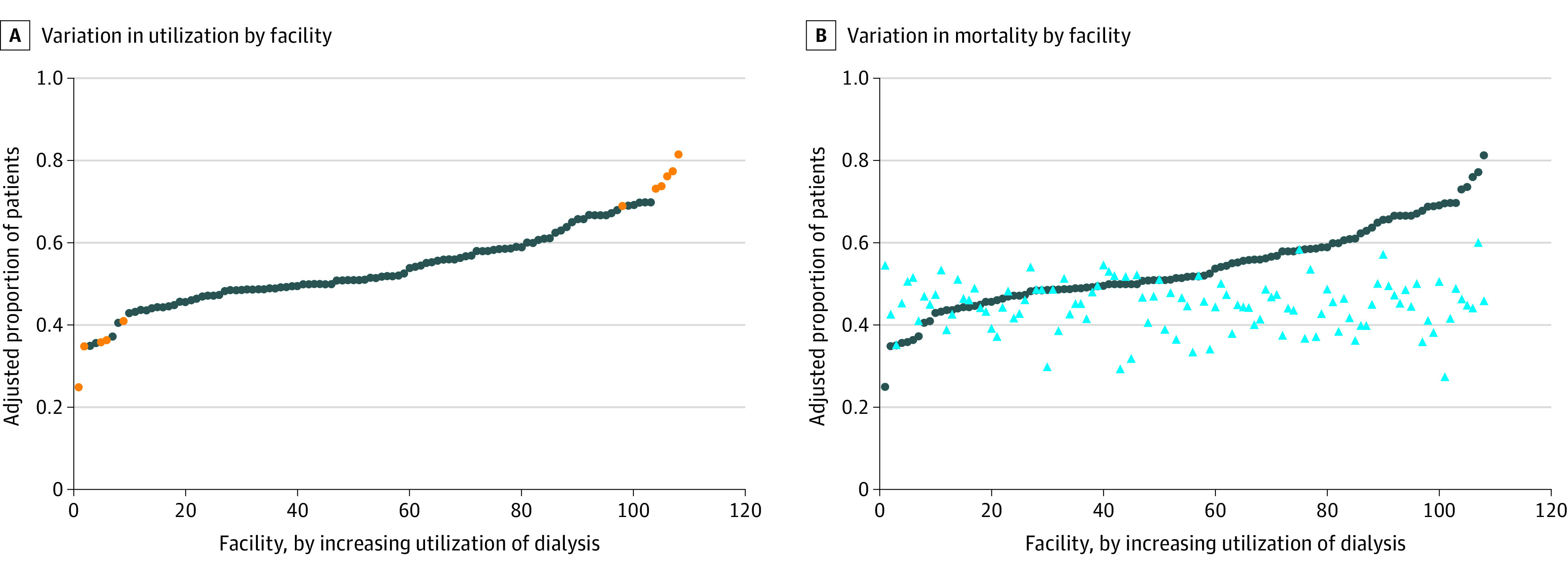
Results: The cohort included 8695 older veterans with a mean (SD) age of 78.8 (7.5) years who were predominantly male (8573 [99%]) and White (6102 [70%]) individuals treated at 108 VA facilities. The observed frequency of dialysis use across facilities ranged from 25.0% to 81.4%, with a median (interquartile range [IQR]) rate of 51.7% (48.4%-60.0%). The observed frequency of mortality across facilities ranged from 27.2% to 60.0%, with a median (IQR) rate of 45.2% (41.2%-48.6%). The median rate ratio (adjusted for multiple patient and facility characteristics) was 1.40 for dialysis use and 1.08 for mortality. The unexplained variation in both outcomes mainly derived from patient characteristics rather than facility characteristics. No correlation was found between dialysis use and mortality at the facility level (correlation coefficient = 0.03).
Conclusions and relevance: This study found sizable variation in dialysis use for older adults that was poorly correlated with facility-level mortality rates and was not accounted for by differences in measured patient and facility characteristics. These findings suggest opportunities to improve the degree to which dialysis use practices align with the values, goals, and preferences of older adults with kidney failure.
Conflict of interest statement
Figures
References
-
- Davison SN, Levin A, Moss AH, et al. ; Kidney Disease: Improving Global Outcomes . Executive summary of the KDIGO Controversies Conference on Supportive Care in Chronic Kidney Disease: developing a roadmap to improving quality care. Kidney Int. 2015;88(3):447-459. doi: 10.1038/ki.2015.110 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
