

Making sense of missense variants in TTN-related congenital myopathies
- PMID: 33449170
- PMCID: PMC7882473
- DOI: 10.1007/s00401-020-02257-0
Making sense of missense variants in TTN-related congenital myopathies
Abstract
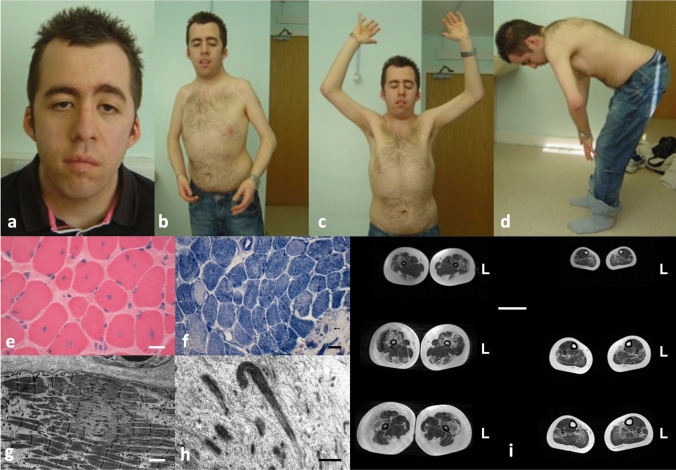
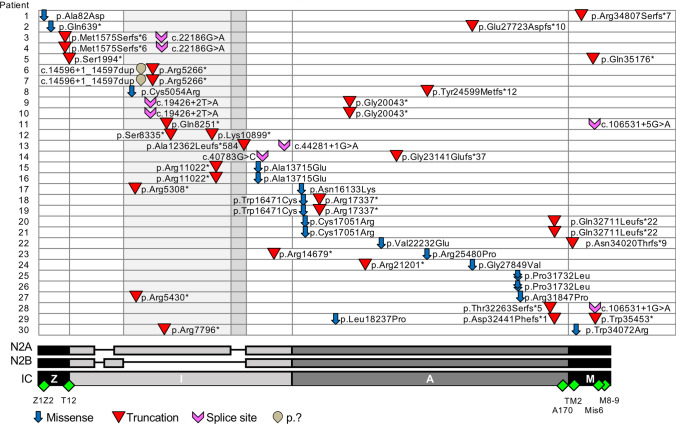
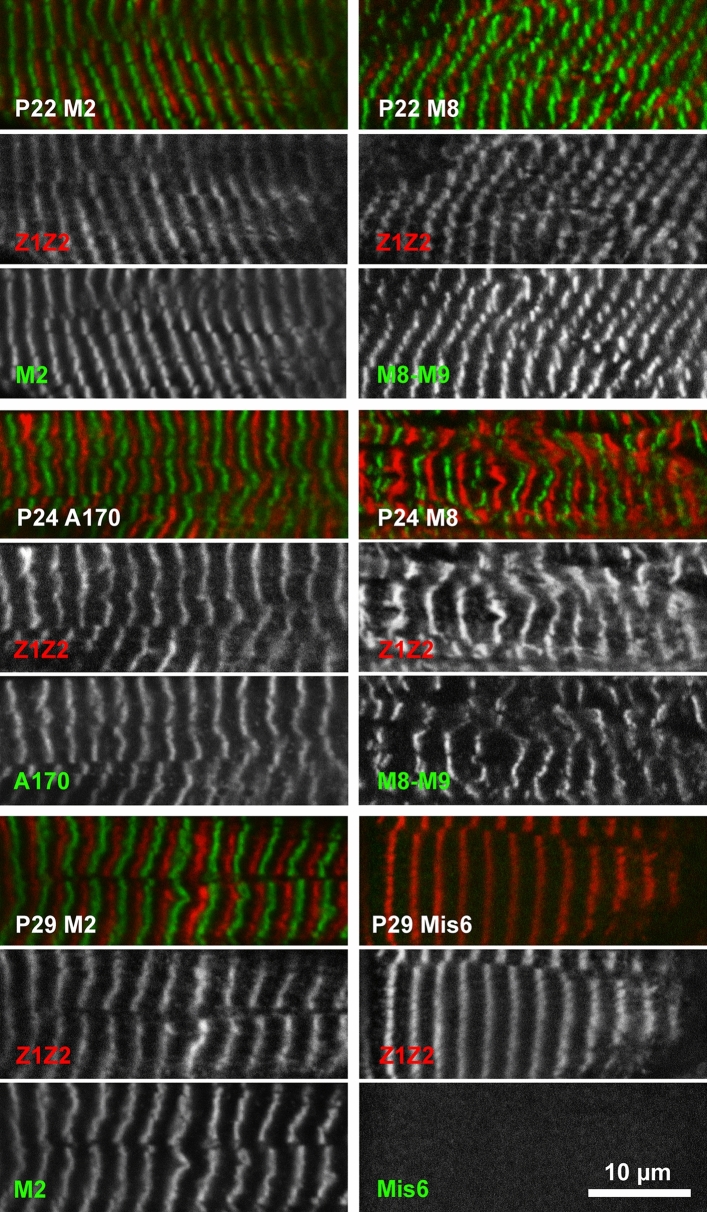
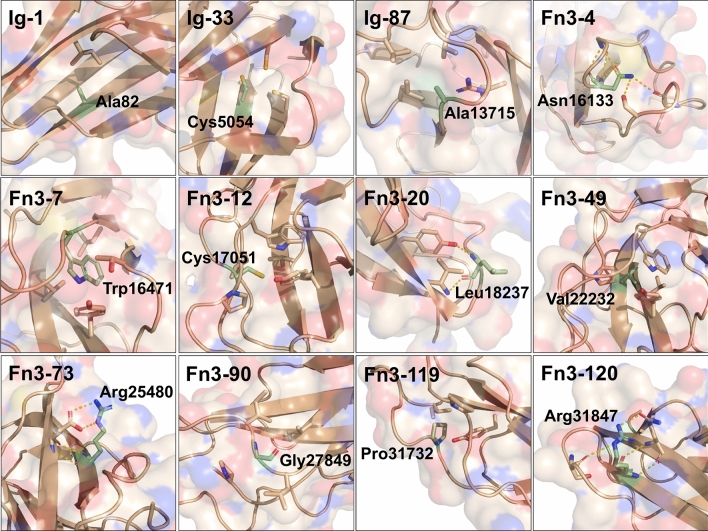
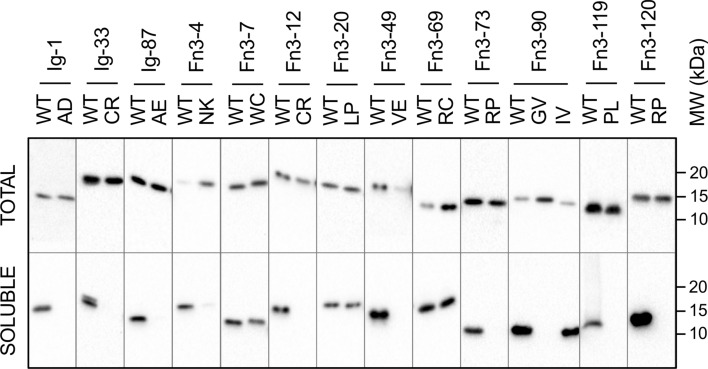
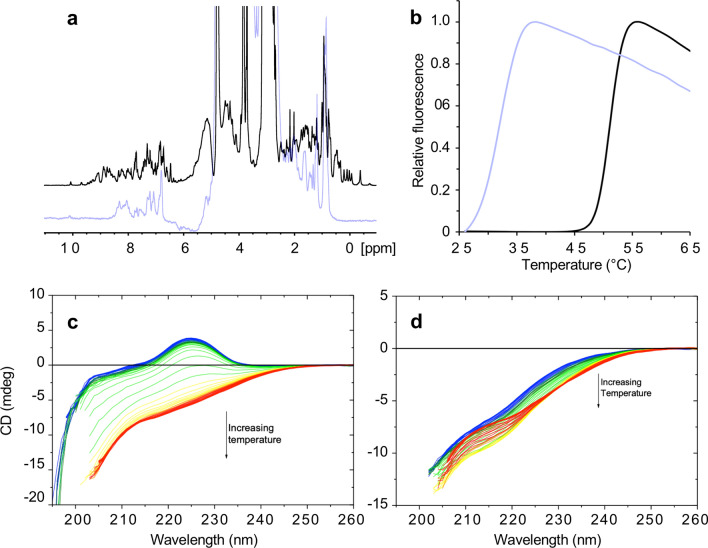
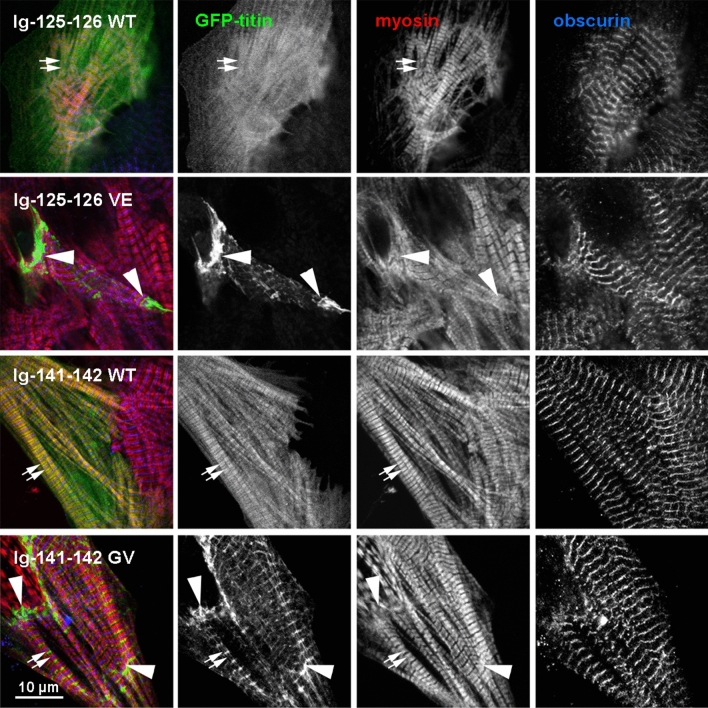
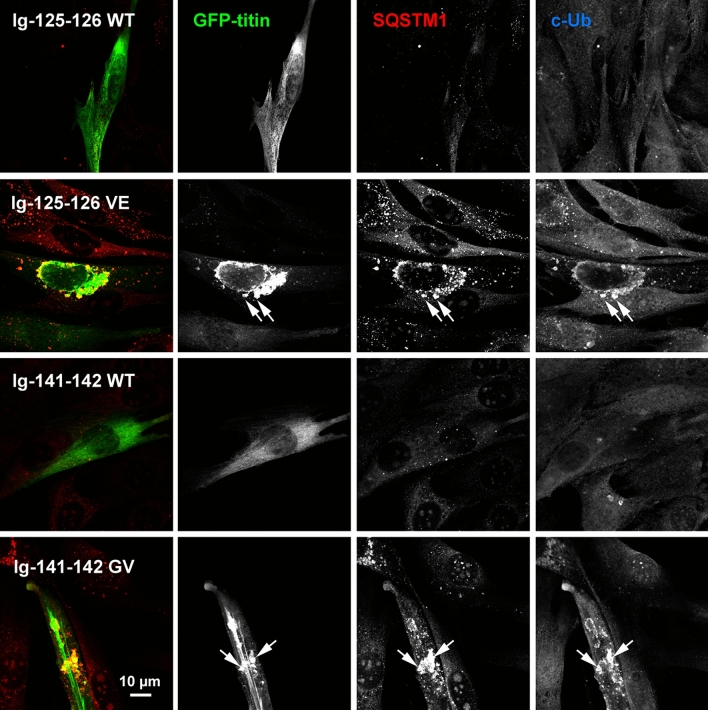
Mutations in the sarcomeric protein titin, encoded by TTN, are emerging as a common cause of myopathies. The diagnosis of a TTN-related myopathy is, however, often not straightforward due to clinico-pathological overlap with other myopathies and the prevalence of TTN variants in control populations. Here, we present a combined clinico-pathological, genetic and biophysical approach to the diagnosis of TTN-related myopathies and the pathogenicity ascertainment of TTN missense variants. We identified 30 patients with a primary TTN-related congenital myopathy (CM) and two truncating variants, or one truncating and one missense TTN variant, or homozygous for one TTN missense variant. We found that TTN-related myopathies show considerable overlap with other myopathies but are strongly suggested by a combination of certain clinico-pathological features. Presentation was typically at birth with the clinical course characterized by variable progression of weakness, contractures, scoliosis and respiratory symptoms but sparing of extraocular muscles. Cardiac involvement depended on the variant position. Our biophysical analyses demonstrated that missense mutations associated with CMs are strongly destabilizing and exert their effect when expressed on a truncating background or in homozygosity. We hypothesise that destabilizing TTN missense mutations phenocopy truncating variants and are a key pathogenic feature of recessive titinopathies that might be amenable to therapeutic intervention.
Figures
Similar articles
-
Two novel mutations in TTN of a patient with congenital myopathy: A case report.Mol Genet Genomic Med. 2019 Aug;7(8):e866. doi: 10.1002/mgg3.866. Epub 2019 Jul 22. Mol Genet Genomic Med. 2019. PMID: 31332964 Free PMC article.
-
Recessive TTN truncating mutations define novel forms of core myopathy with heart disease.Hum Mol Genet. 2014 Feb 15;23(4):980-91. doi: 10.1093/hmg/ddt494. Epub 2013 Oct 8. Hum Mol Genet. 2014. PMID: 24105469 Free PMC article.
-
Recessive truncating titin gene, TTN, mutations presenting as centronuclear myopathy.Neurology. 2013 Oct 1;81(14):1205-14. doi: 10.1212/WNL.0b013e3182a6ca62. Epub 2013 Aug 23. Neurology. 2013. PMID: 23975875 Free PMC article.
-
Increasing Role of Titin Mutations in Neuromuscular Disorders.J Neuromuscul Dis. 2016 Aug 30;3(3):293-308. doi: 10.3233/JND-160158. J Neuromuscul Dis. 2016. PMID: 27854229 Free PMC article. Review.
-
Approach to the diagnosis of congenital myopathies.Neuromuscul Disord. 2014 Feb;24(2):97-116. doi: 10.1016/j.nmd.2013.11.003. Epub 2013 Nov 18. Neuromuscul Disord. 2014. PMID: 24456932 Free PMC article.
Cited by
-
Protein haploinsufficiency drivers identify MYBPC3 variants that cause hypertrophic cardiomyopathy.J Biol Chem. 2021 Jul;297(1):100854. doi: 10.1016/j.jbc.2021.100854. Epub 2021 Jun 5. J Biol Chem. 2021. PMID: 34097875 Free PMC article.
-
TTN-related hereditary myopathy with early respiratory failure presented with elevated hemoglobin initially: A case report and literature review.Heliyon. 2024 Apr 12;10(8):e29637. doi: 10.1016/j.heliyon.2024.e29637. eCollection 2024 Apr 30. Heliyon. 2024. PMID: 38655354 Free PMC article.
-
Reanalysis of RNA sequencing data ends diagnostic odyssey and expands the phenotypic spectrum of congenital titinopathy.Am J Med Genet A. 2024 Nov;194(11):e63798. doi: 10.1002/ajmg.a.63798. Epub 2024 Jun 24. Am J Med Genet A. 2024. PMID: 38924341 Free PMC article.
-
Structure determination and analysis of titin A-band fibronectin type III domains provides insights for disease-linked variants and protein oligomerisation.J Struct Biol. 2023 Sep;215(3):108009. doi: 10.1016/j.jsb.2023.108009. Epub 2023 Aug 5. J Struct Biol. 2023. PMID: 37549721 Free PMC article.
-
Basic science methods for the characterization of variants of uncertain significance in hypertrophic cardiomyopathy.Front Cardiovasc Med. 2023 Aug 1;10:1238515. doi: 10.3389/fcvm.2023.1238515. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37600050 Free PMC article. Review.
References
-
- Bang ML, Centner T, Fornoff F, Geach AJ, Gotthardt M, McNabb M, et al. The complete gene sequence of titin, expression of an unusual approximately 700-kDa titin isoform, and its interaction with obscurin identify a novel Z-line to I-band linking system. Circ Res. 2001;89:1065–1072. doi: 10.1161/hh2301.100981. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
