

Rectal cancer with complete endoscopic response after neoadjuvant therapy: what is the meaning of a positive MRI?
- PMID: 33449186
- PMCID: PMC8222060
- DOI: 10.1007/s00330-020-07657-0
Rectal cancer with complete endoscopic response after neoadjuvant therapy: what is the meaning of a positive MRI?
Abstract
Objectives: To determine the short-term outcomes of discordant tumor assessments between DWI-MRI and endoscopy in patients with treated rectal cancer when tumor-bed diffusion restriction is present ("+DWI").
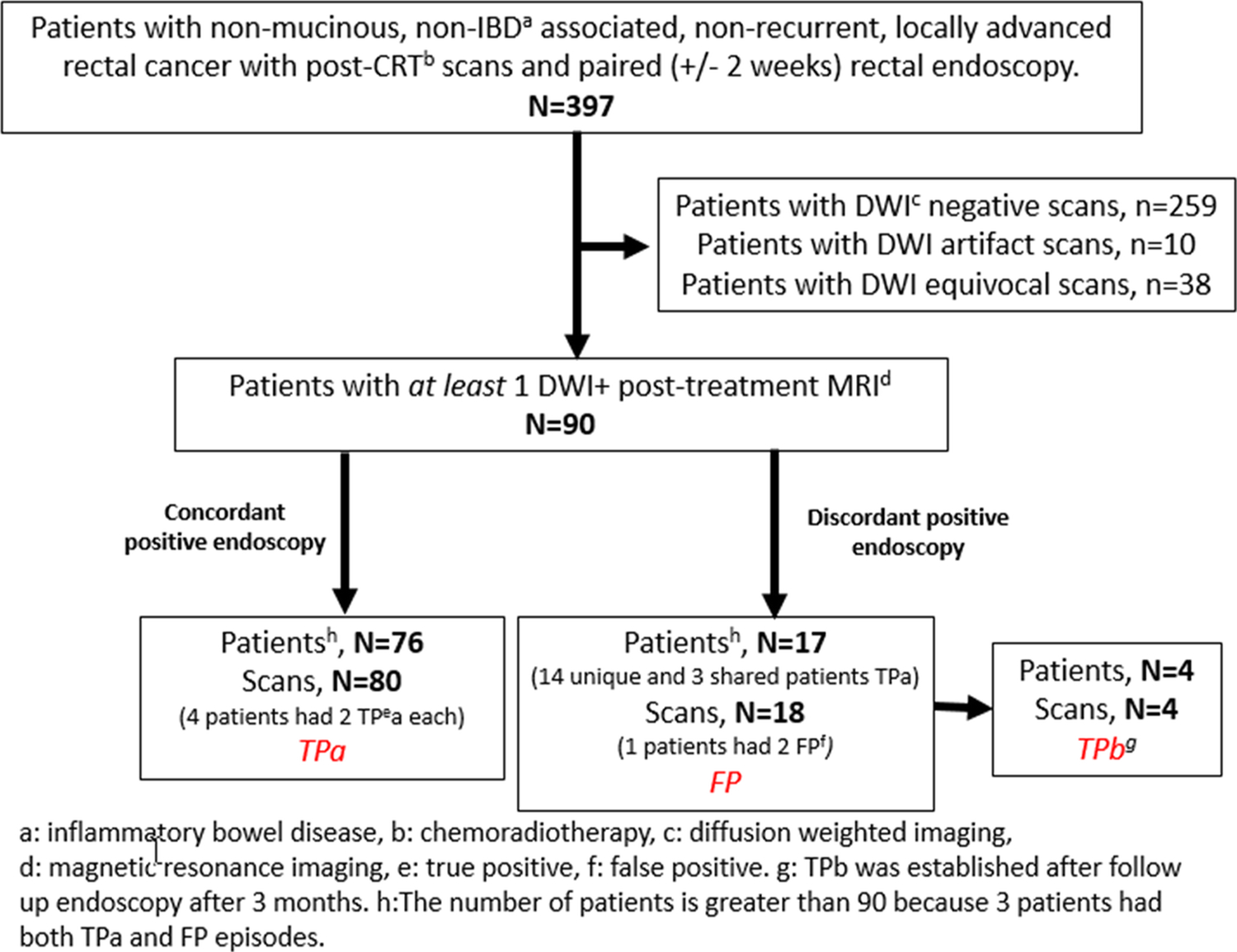
Methods: In this HIPPA-compliant, IRB-approved retrospective study, rectal MRI and endoscopic reports were reviewed for patients with locally advanced primary rectal adenocarcinoma (LARC) treated with chemoradiotherapy or total neoadjuvant therapy and imaged between January 2016 and December 2019. Eligible patients had a +DWI and endoscopy within 2 weeks of each other. True positive MRI were those with tumor on endoscopy and/or biopsy (TPa) or in whom endoscopy was negative for tumor, but subsequent 3-month follow-up endoscopy and DWI were both positive (TPb). The positive predictive value of DWI-MRI was calculated on a per-scan and per-patient basis. DWI-negative MRI exams were not explored in this study.
Results: In total, 397 patients with nonmetastatic primary LARC were analyzed. After exclusions, 90 patients had 98 follow-up rectal MRI studies with +DWI. Seventy-six patients underwent 80 MRI scans and had concordant findings at endoscopy (TPa). Seventeen patients underwent 18 MRI scans and had discordant findings at endoscopy (FP); among these, 4 scans in 4 patients were initially false positive (FP) but follow-up MRI remained +DWI and the endoscopy turned concordantly positive (TPb). PPV was 0.86 per scan and per patient. In 4/18 (22%) scans and 4/17 (24%) patients with discordances, MRI detected tumor regrowth before endoscopy.
Conclusions: Although most +DWI exams discordant with endoscopy are false positive, 22% will reveal that DWI-MRI detects tumor recurrence before endoscopy.
Key points: • Most often, in post-treatment assessment for rectal cancer when DWI-MRI shows restriction in the tumor bed and endoscopy shows no tumor, +DWI MRI will be proven false positive. • Conversely, our study demonstrated that, allowing for sequential follow-up at a 3-month maximum interval, DWI-MRI may detect tumor presence in the treated tumor bed before endoscopy in 22% of discordant findings between DWI-MRI and endoscopy. • Our results showed that a majority of DWI-MRI-positive scans in treated rectal cancer concur with the presence of tumor on endoscopy performed within 2 weeks.
Keywords: MRI, functional; Rectal cancer; Surgical endoscopy.
Conflict of interest statement
Conflict of Interest:
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures
References
-
- Maas M, Beets-Tan RG, Lambregts DM et al. (2011) Wait-and-see policy for clinical complete responders after chemoradiation for rectal cancer. J Clin Oncol 29:4633–4640 - PubMed
-
- Habr-Gama A, Perez RO, Proscurshim I et al. (2006) Patterns of failure and survival for nonoperative treatment of stage c0 distal rectal cancer following neoadjuvant chemoradiation therapy. J Gastrointest Surg 10:1319–1328; discussion 1328–1319 - PubMed
-
- Habr-Gama A, Gama-Rodrigues J, Sao Juliao GP et al. (2014) Local recurrence after complete clinical response and watch and wait in rectal cancer after neoadjuvant chemoradiation: impact of salvage therapy on local disease control. Int J Radiat Oncol Biol Phys 88:822–828 - PubMed
-
- Smith JD, Ruby JA, Goodman KA et al. (2012) Nonoperative management of rectal cancer with complete clinical response after neoadjuvant therapy. Ann Surg 256:965–972 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
