

Phase II Trial of Costimulation Blockade With Abatacept for Prevention of Acute GVHD
- PMID: 33449816
- PMCID: PMC8260909
- DOI: 10.1200/JCO.20.01086
Phase II Trial of Costimulation Blockade With Abatacept for Prevention of Acute GVHD
Abstract
Purpose: Severe (grade 3-4) acute graft-versus-host disease (AGVHD) is a major cause of death after unrelated-donor (URD) hematopoietic cell transplant (HCT), resulting in particularly high mortality after HLA-mismatched transplantation. There are no approved agents for AGVHD prevention, underscoring the critical unmet need for novel therapeutics. ABA2 was a phase II trial to rigorously assess safety, efficacy, and immunologic effects of adding T-cell costimulation blockade with abatacept to calcineurin inhibitor (CNI)/methotrexate (MTX)-based GVHD prophylaxis, to test whether abatacept could decrease AGVHD.
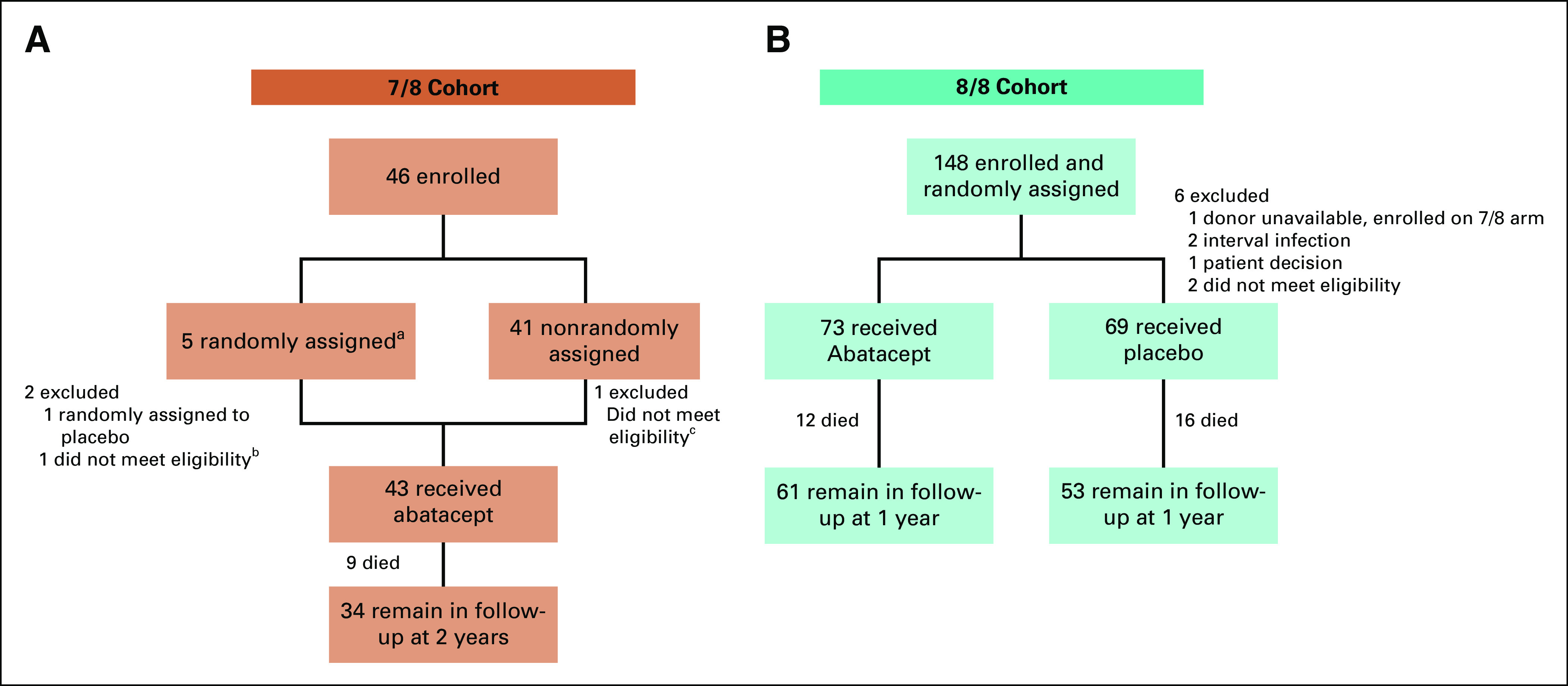
Methods: ABA2 enrolled adults and children with hematologic malignancies under two strata: a randomized, double-blind, placebo-controlled stratum (8/8-HLA-matched URD), comparing CNI/MTX plus abatacept with CNI/MTX plus placebo, and a single-arm stratum (7/8-HLA-mismatched URD) comparing CNI/MTX plus abatacept versus CNI/MTX CIBMTR controls. The primary end point was day +100 grade 3-4 AGVHD, with day +180 severe-AGVHD-free-survival (SGFS) a key secondary end point. Sample sizes were calculated using a higher type-1 error (0.2) as recommended for phase II trials, and were based on predicting that abatacept would reduce grade 3-4 AGVHD from 20% to 10% (8/8s) and 30% to 10% (7/8s). ABA2 enrolled 142 recipients (8/8s, median follow-up = 716 days) and 43 recipients (7/8s, median follow-up = 708 days).
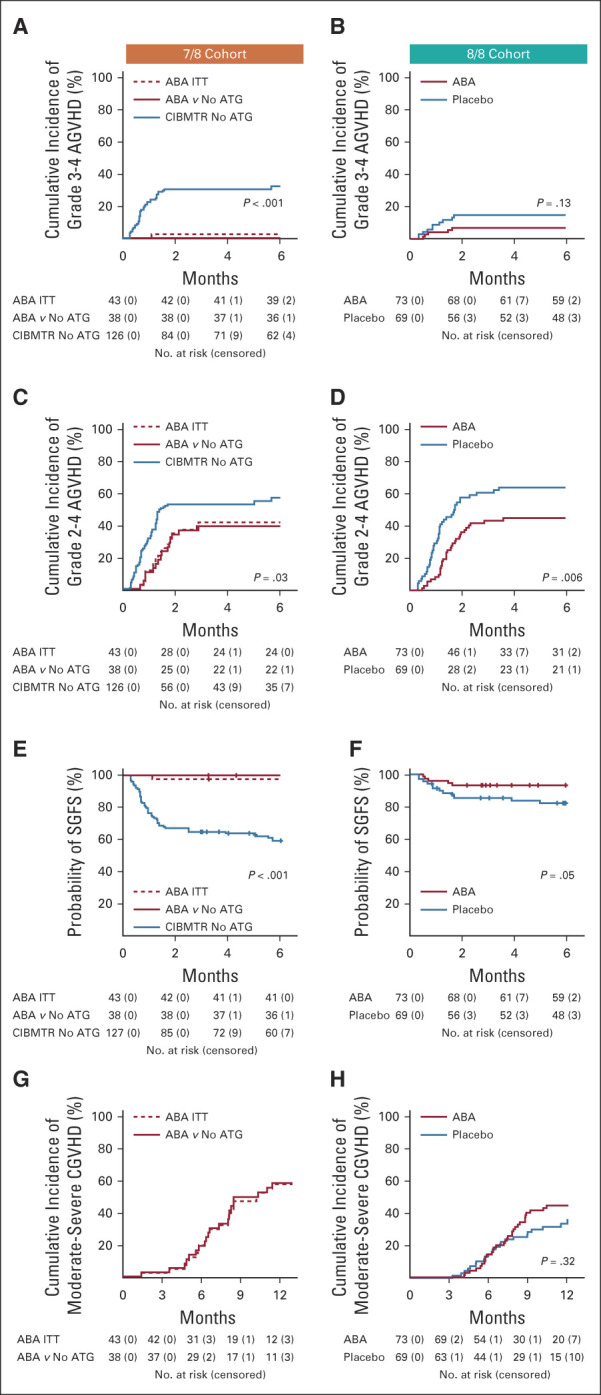
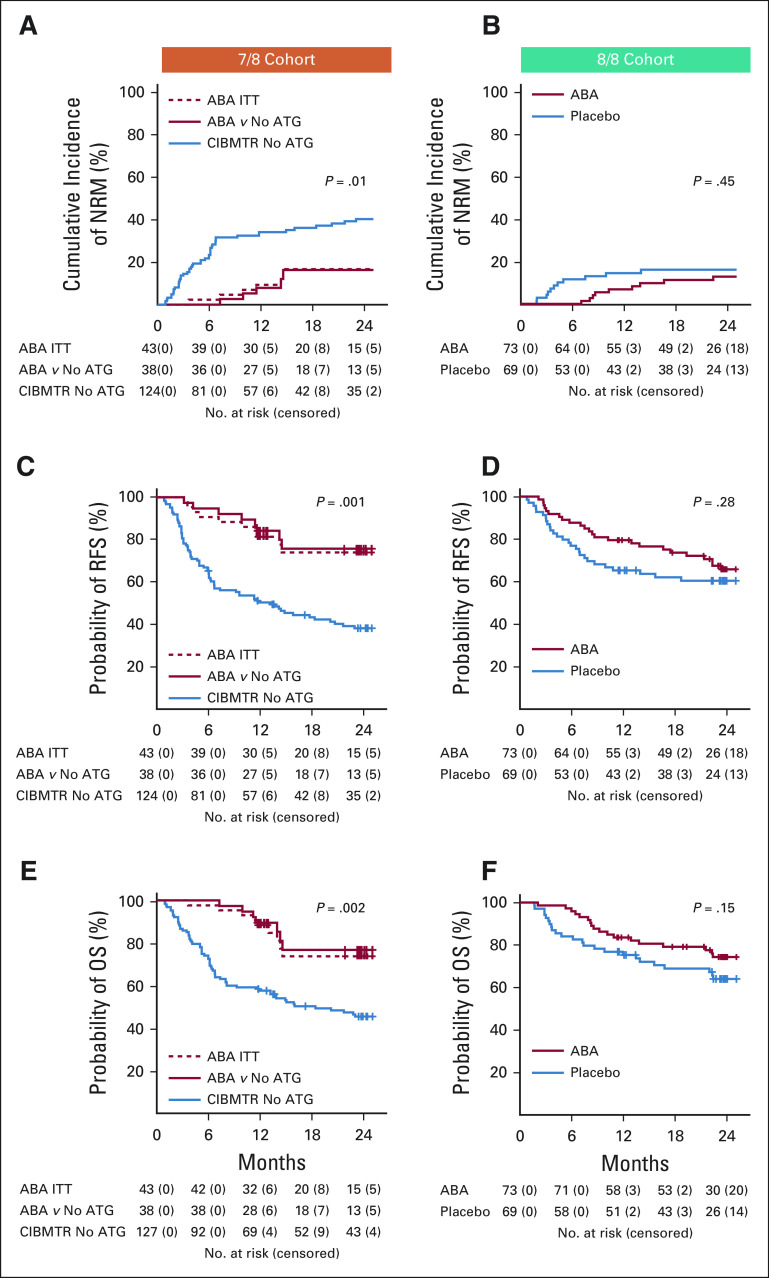
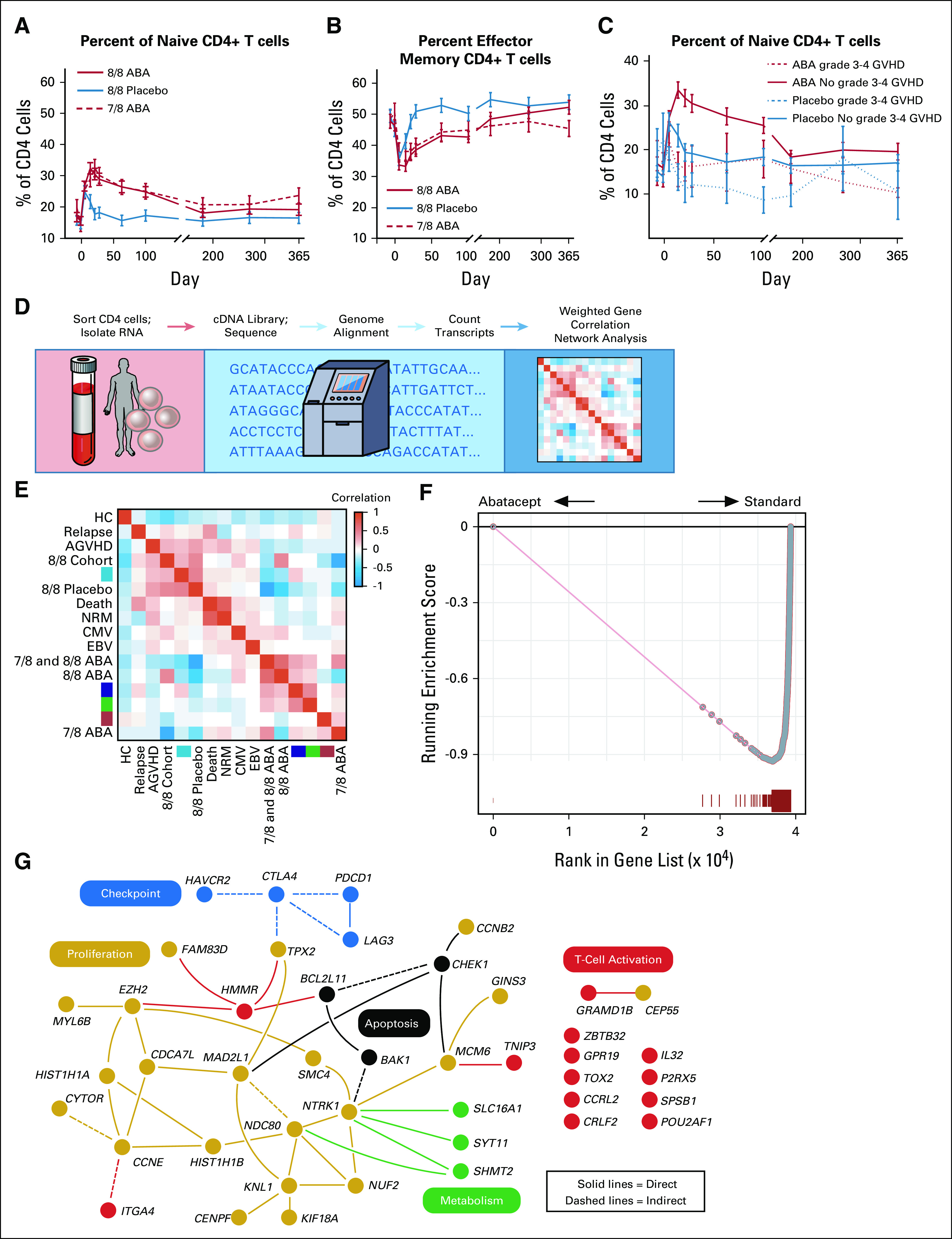
Results: In 8/8s, grade 3-4 AGVHD was 6.8% (abatacept) versus 14.8% (placebo) (P = .13, hazard ratio = 0.45). SGFS was 93.2% (CNI/MTX plus abatacept) versus 82% (CNI/MTX plus placebo, P = .05). In the smaller 7/8 cohort, grade 3-4 AGVHD was 2.3% (CNI/MTX plus abatacept, intention-to-treat population), which compared favorably with a nonrandomized matched cohort of CNI/MTX (30.2%, P < .001), and the SGFS was better (97.7% v 58.7%, P < .001). Immunologic analysis revealed control of T-cell activation in abatacept-treated patients.
Conclusion: Adding abatacept to URD HCT was safe, reduced AGVHD, and improved SGFS. These results suggest that abatacept may substantially improve AGVHD-related transplant outcomes, with a particularly beneficial impact on HLA-mismatched HCT.
Conflict of interest statement
Figures
References
-
- Bunin N, Carston M, Wall D, et al. Unrelated marrow transplantation for children with acute lymphoblastic leukemia in second remission Blood 993151–31572002 - PubMed
-
- Lee SJ, Klein J, Haagenson M, et al. High-resolution donor-recipient HLA matching contributes to the success of unrelated donor marrow transplantation Blood 1104576–45832007 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 HL095791/HL/NHLBI NIH HHS/United States
- P01 CA065493/CA/NCI NIH HHS/United States
- R01 HL118979/HL/NHLBI NIH HHS/United States
- R01 HL147324/HL/NHLBI NIH HHS/United States
- R37 AI034495/AI/NIAID NIH HHS/United States
- R01 HL056067/HL/NHLBI NIH HHS/United States
- UG1 HL069254/HL/NHLBI NIH HHS/United States
- P01 CA039542/CA/NCI NIH HHS/United States
- KL2 TR000455/TR/NCATS NIH HHS/United States
- R01 FD004099/FD/FDA HHS/United States
- P01 AI056299/AI/NIAID NIH HHS/United States
- K23 HL136900/HL/NHLBI NIH HHS/United States
- R01 HL155114/HL/NHLBI NIH HHS/United States
- K12 HD072245/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
