

Risk-Based Selection of Individuals for Oral Cancer Screening
- PMID: 33449824
- PMCID: PMC8189638
- DOI: 10.1200/JCO.20.02855
Risk-Based Selection of Individuals for Oral Cancer Screening
Abstract
Purpose: We evaluated proof of principle for resource-efficient, risk-based screening through reanalysis of the Kerala Oral Cancer Screening Trial.
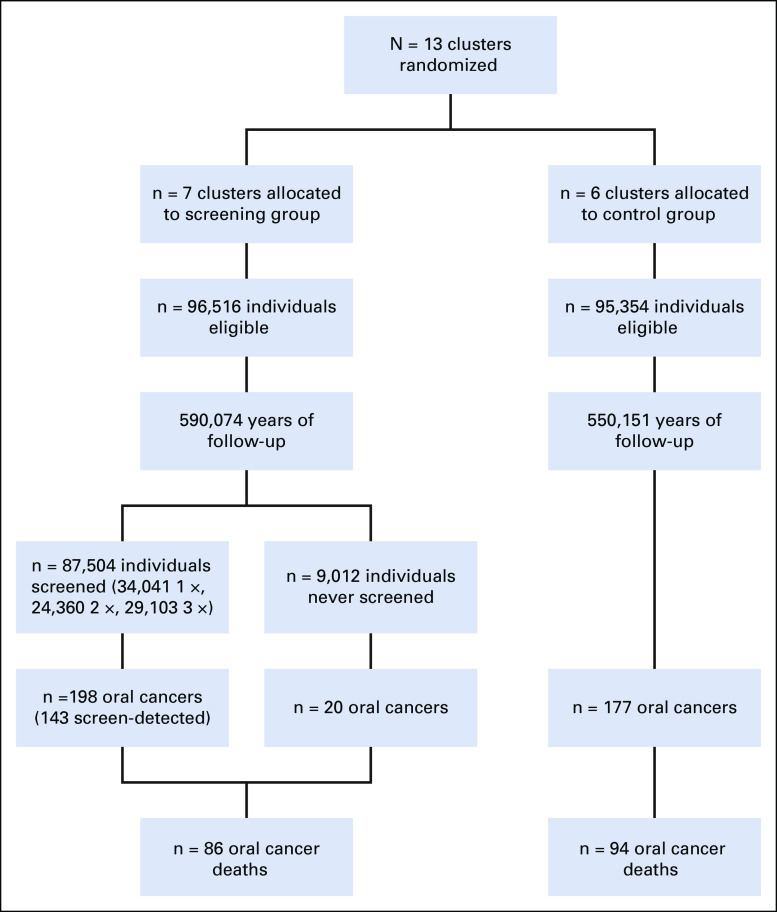
Methods: The cluster-randomized trial included three triennial rounds of visual inspection (seven clusters, n = 96,516) versus standard of care (six clusters, n = 95,354) and up to 9 years of follow-up. We developed a Cox regression-based risk prediction model for oral cancer incidence. Using this risk prediction model to adjust for the oral cancer risk imbalance between arms, through intention-to-treat (ITT) analyses that accounted for cluster randomization, we calculated the relative (hazard ratios [HRs]) and absolute (rate differences [RDs]) screening efficacy on oral cancer mortality and compared screening efficiency across risk thresholds.
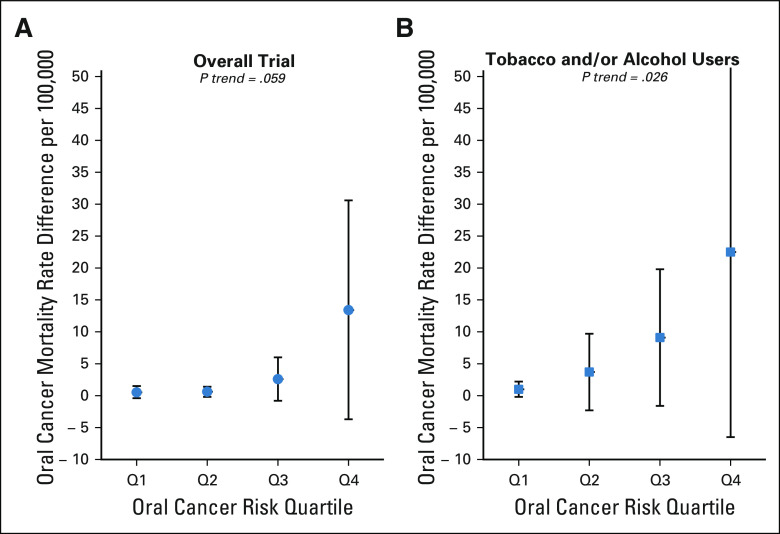
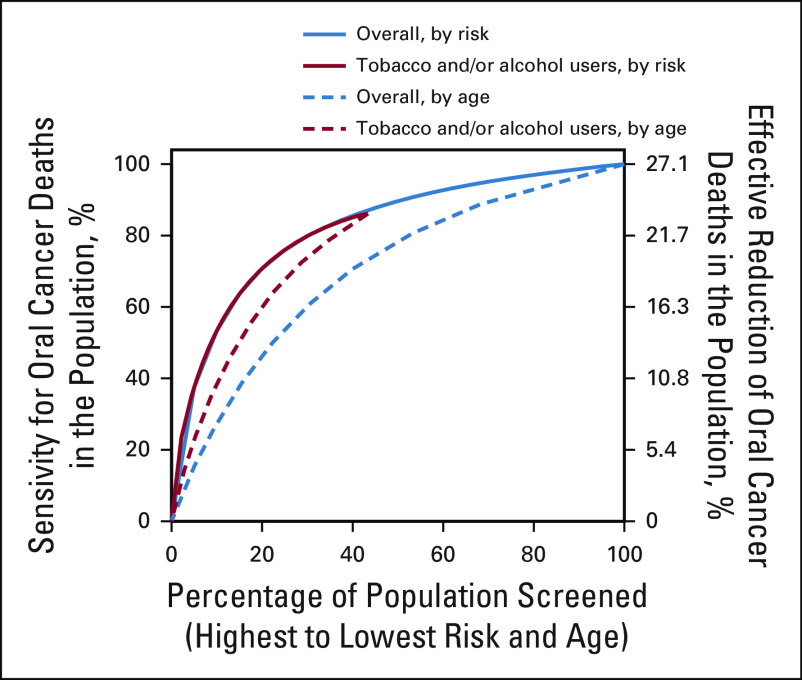
Results: Oral cancer mortality was reduced by 27% in the screening versus control arms (HR = 0.73; 95% CI, 0.54 to 0.98), including a 29% reduction in ever-tobacco and/or ever-alcohol users (HR = 0.71; 95% CI, 0.51 to 0.99). This relative efficacy was similar across oral cancer risk quartiles (P interaction = .59); consequently, the absolute efficacy increased with increasing model-predicted risk-overall trial: RD in the lowest risk quartile (Q1) = 0.5/100,000 versus 13.4/100,000 in the highest quartile (Q4), P trend = .059 and ever-tobacco and/or ever-alcohol users: Q1 RD = 1.0/100,000 versus Q4 = 22.5/100,000; P trend = .026. In a population akin to the Kerala trial, screening of 100% of individuals would provide 27.1% oral cancer mortality reduction at number needed to screen (NNS) = 2,043. Restriction of screening to ever-tobacco and/or ever-alcohol users with no additional risk stratification would substantially enhance efficiency (43.4% screened for 23.3% oral cancer mortality reduction at NNS = 1,029), whereas risk prediction model-based screening of 50% of ever-tobacco and/or ever-alcohol users at highest risk would further enhance efficiency with little loss in program sensitivity (21.7% screened for 19.7% oral cancer mortality reduction at NNS = 610).
Conclusion: In the Kerala trial, the efficacy of oral cancer screening was greatest in individuals at highest oral cancer risk. These results provide proof of principle that risk-based oral cancer screening could substantially enhance the efficiency of screening programs.
Trial registration: ClinicalTrials.gov NCT04494620.
Figures
Comment in
-
Risk-based oral cancer screening - lessons to be learnt.Nat Rev Clin Oncol. 2021 Aug;18(8):471-472. doi: 10.1038/s41571-021-00511-2. Nat Rev Clin Oncol. 2021. PMID: 33883701 Free PMC article.
References
-
- Shield KD, Ferlay J, Jemal A, et al. The global incidence of lip, oral cavity, and pharyngeal cancers by subsite in 2012. CA Cancer J Clin. 2017;67:51–64. - PubMed
-
- Sankaranarayanan R, Ramadas K, Amarasinghe H, et al. Oral cancer: Prevention, early detection, and treatment. In: Gelband H, Jha P, Sankaranarayanan R, et al., editors. Cancer: Disease Control Priorities. ed 3. Volume 3. Washington, DC: The International Bank for Reconstruction and Development/The World Bank; 2015. - PubMed
-
- Sankaranarayanan R, Ramadas K, Thomas G, et al. Effect of screening on oral cancer mortality in Kerala, India: A cluster-randomised controlled trial. Lancet. 2005;365:1927–1933. - PubMed
-
- Ramadas K, Sankaranarayanan R, Jacob BJ, et al. Interim results from a cluster randomized controlled oral cancer screening trial in Kerala, India. Oral Oncol. 2003;39:580–588. - PubMed
-
- Sankaranarayanan R, Ramadas K, Thara S, et al. Long term effect of visual screening on oral cancer incidence and mortality in a randomized trial in Kerala, India. Oral Oncol. 2013;49:314–321. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
