

Association of digoxin with mortality in patients with advanced chronic kidney disease: A population-based cohort study
- PMID: 33449946
- PMCID: PMC7810292
- DOI: 10.1371/journal.pone.0245620
Association of digoxin with mortality in patients with advanced chronic kidney disease: A population-based cohort study
Abstract
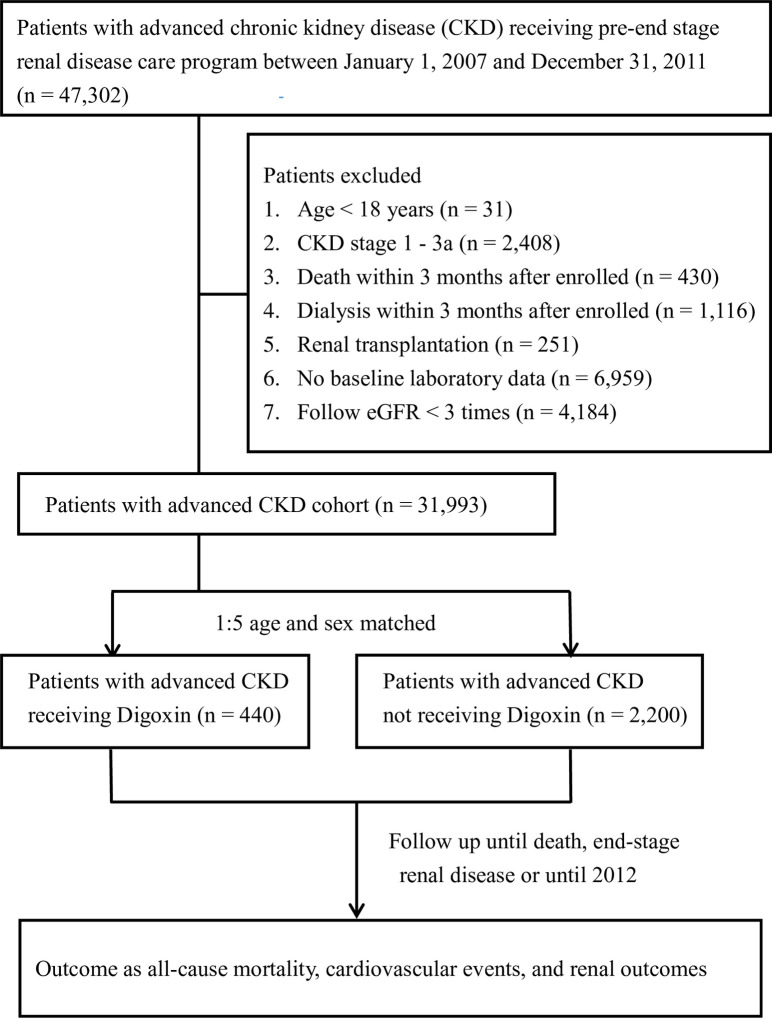
Digoxin is commonly prescribed for heart failure and atrial fibrillation, but there is limited data on its safety in patients with chronic kidney disease (CKD). We conducted a population-based cohort study using the pre-end stage renal disease (ESRD) care program registry and the National Health Insurance Research Database in Taiwan. Of advanced CKD patient cohort (N = 31,933), we identified the digoxin user group (N = 400) matched with age and sex non-user group (N = 2,220). Multivariable Cox proportional hazards and sub-distribution hazards models were used to evaluate the association between digoxin use and the risk of death, cardiovascular events (acute coronary syndrome, ischemic stroke, or hemorrhagic stroke) and renal outcomes (ESRD, rapid decline in estimated glomerular filtration rate-eGFR, or acute kidney injury). Results showed that all-cause mortality was higher in the digoxin user group than in the non-user group, after adjusting for covariates (adjusted hazard ratio, aHR 1.63; 95% CI 1.23-2.17). The risk for acute coronary syndrome (sub-distribution hazard ratio, sHR 1.18; 95% CI 0.75-1.86), ischemic stroke (sHR 1.42; 95% CI 0.85-2.37), and rapid eGFR decline (sHR 1.00 95% CI 0.78-1.27) was not significantly different between two groups. In conclusion, our study demonstrated that digoxin use was associated with increased mortality, but not cardiovascular events or renal function decline in advanced CKD patients. This finding warns the safety of prescribing digoxin in this population. Future prospective studies are needed to overcome the limitations of cohort study design.
Conflict of interest statement
Co-author Ping-Hsun Wu is a fellow of PLOS ONE Editorial Board Members. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Similar articles
-
Association between the risk of heart failure hospitalization and end-stage renal disease with digoxin usage in patients with cardiorenal syndrome: A population-based study.Front Public Health. 2023 Jan 17;10:1074017. doi: 10.3389/fpubh.2022.1074017. eCollection 2022. Front Public Health. 2023. PMID: 36733284 Free PMC article.
-
Effect of spironolactone on the risks of mortality and hospitalization for heart failure in pre-dialysis advanced chronic kidney disease: A nationwide population-based study.Int J Cardiol. 2017 Jul 1;238:72-78. doi: 10.1016/j.ijcard.2017.03.080. Epub 2017 Mar 18. Int J Cardiol. 2017. PMID: 28363684
-
Warfarin, kidney dysfunction, and outcomes following acute myocardial infarction in patients with atrial fibrillation.JAMA. 2014 Mar 5;311(9):919-28. doi: 10.1001/jama.2014.1334. JAMA. 2014. PMID: 24595776
-
Comparison of incidence of acute kidney injury, chronic kidney disease and end-stage renal disease between atrial fibrillation and atrial flutter: real-world evidences from a propensity score-matched national cohort analysis.Intern Emerg Med. 2019 Oct;14(7):1113-1118. doi: 10.1007/s11739-019-02089-1. Epub 2019 May 9. Intern Emerg Med. 2019. PMID: 31073825
-
Increased risk of mortality in the elderly population with late-stage chronic kidney disease: a cohort study in Taiwan.Nephrol Dial Transplant. 2008 Oct;23(10):3192-8. doi: 10.1093/ndt/gfn222. Epub 2008 May 1. Nephrol Dial Transplant. 2008. PMID: 18450830
Cited by
-
An Updated Review of the Management of Chronic Heart Failure in Patients with Chronic Kidney Disease.Rev Cardiovasc Med. 2024 Apr 11;25(4):144. doi: 10.31083/j.rcm2504144. eCollection 2024 Apr. Rev Cardiovasc Med. 2024. PMID: 39076544 Free PMC article. Review.
-
Identification of core genes and pathways between geriatric multimorbidity and renal insufficiency: potential therapeutic agents discovered using bioinformatics analysis.BMC Med Genomics. 2022 Oct 8;15(1):212. doi: 10.1186/s12920-022-01370-1. BMC Med Genomics. 2022. PMID: 36209090 Free PMC article.
-
Atrial Fibrillation and Chronic Kidney Disease: Aetiology and Management.Rev Cardiovasc Med. 2024 Apr 9;25(4):143. doi: 10.31083/j.rcm2504143. eCollection 2024 Apr. Rev Cardiovasc Med. 2024. PMID: 39076563 Free PMC article. Review.
-
Association of Kidney Function With Risk of Adverse Effects of Therapies for Atrial Fibrillation.Kidney Int Rep. 2022 Dec 13;8(3):606-618. doi: 10.1016/j.ekir.2022.12.002. eCollection 2023 Mar. Kidney Int Rep. 2022. PMID: 36938096 Free PMC article.
-
Atrial Fibrillation in Chronic Kidney Disease: An Overview.Cureus. 2022 Aug 7;14(8):e27753. doi: 10.7759/cureus.27753. eCollection 2022 Aug. Cureus. 2022. PMID: 36106212 Free PMC article. Review.
References
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016; 37(27):2129–200. 10.1093/eurheartj/ehw128 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
