

Acute kidney injury after in-hospital cardiac arrest
- PMID: 33450335
- PMCID: PMC7902429
- DOI: 10.1016/j.resuscitation.2020.12.023
Acute kidney injury after in-hospital cardiac arrest
Abstract
Aim: Determine 1) frequency and risk factors for acute kidney injury (AKI) after in-hospital cardiac arrest (IHCA) in the Therapeutic Hypothermia after Pediatric Cardiac Arrest In-Hospital (THAPCA-IH) trial and associated outcomes; 2) impact of temperature management on post-IHCA AKI.
Methods: Secondary analysis of THAPCA-IH; a randomized controlled multi-national trial at 37 children's hospitals.
Eligibility: Serum creatinine (Cr) within 24 h of randomization.
Outcomes: Prevalence of severe AKI defined by Stage 2 or 3 Kidney Disease Improving Global Outcomes Cr criteria. 12-month survival with favorable neurobehavioral outcome. Analyses stratified by entire cohort and cardiac subgroup. Risk factors and outcomes compared among cohorts with and without severe AKI.
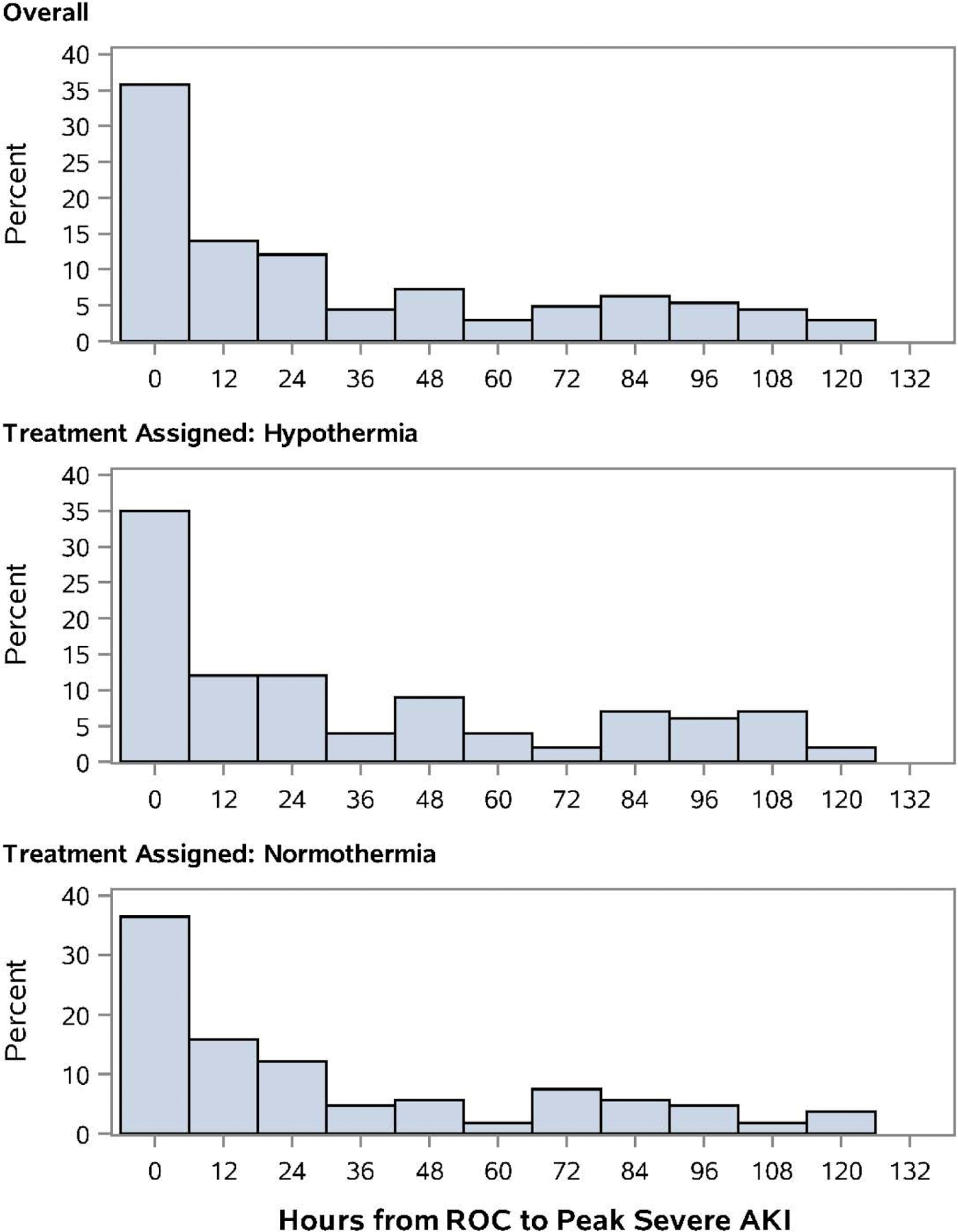
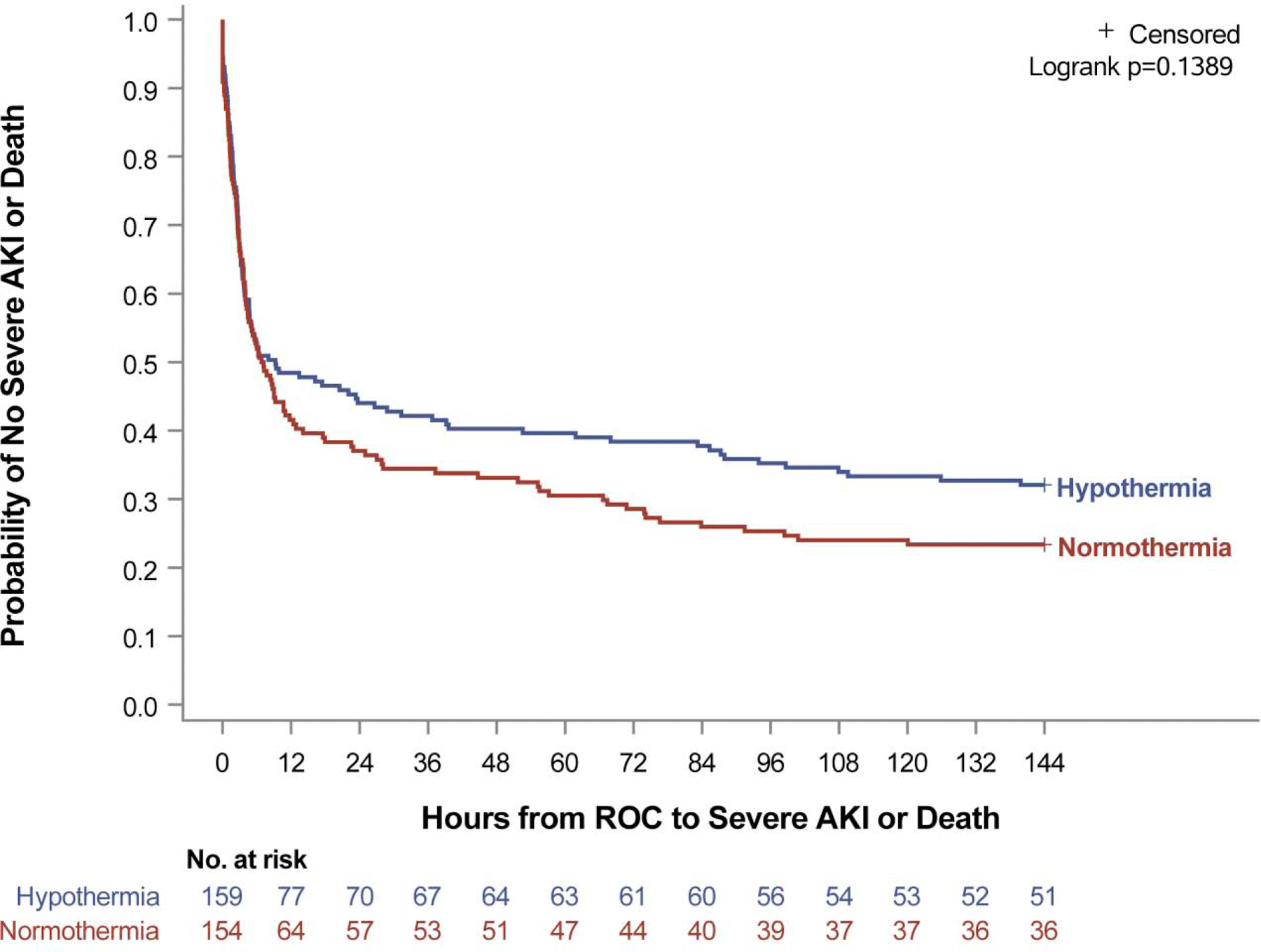
Results: Subject randomization: 159 to hypothermia, 154 to normothermia. Overall, 80% (249) developed AKI (any stage), and 66% (207) developed severe AKI. Cardiac patients (204, 65%) were more likely to develop severe AKI (72% vs 56%,p = 0.006). Preexisting cardiac or renal conditions, baseline lactate, vasoactive support, and systolic blood pressure were associated with severe AKI. Comparing hypothermia versus normothermia, there were no differences in severe AKI rate (63% vs 70%,p = 0.23), peak Cr, time to peak Cr, or freedom from mortality or severe AKI (p = 0.14). Severe AKI was associated with decreased hospital survival (48% vs 65%,p = 0.006) and decreased 12-month survival with favorable neurobehavioral outcome (30% vs 53%,p < 0.001).
Conclusion: Severe post-IHCA AKI occurred frequently especially in those with preexisting cardiac or renal conditions and peri-arrest hemodynamic instability. Severe AKI was associated with decreased survival with favorable neurobehavioral outcome. Hypothermia did not decrease incidence of severe AKI post-IHCA.
Keywords: Acute kidney injury; In-Hospital; Post-Cardiac arrest; Therapeutic hypothermia.
Copyright © 2021 Elsevier B.V. All rights reserved.
Conflict of interest statement
Conflicts of interest:
The views expressed in this article are solely those of the authors and do not necessarily represent the official views of the National Heart, Lung, and Blood Institute or the National Institutes of Health.
Figures
Comment in
-
Reply to: Acute kidney injury after in-hospital pediatric cardiac arrest To the Editor.Resuscitation. 2021 Jun;163:209-210. doi: 10.1016/j.resuscitation.2021.04.022. Epub 2021 Apr 27. Resuscitation. 2021. PMID: 33930502 No abstract available.
-
Acute kidney injury after in-hospital pediatric cardiac arrest.Resuscitation. 2021 Jun;163:207-208. doi: 10.1016/j.resuscitation.2021.03.037. Epub 2021 May 12. Resuscitation. 2021. PMID: 33965473 No abstract available.
References
-
- Neumar RW, Nolan JP, Adrie C, et al. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A consensus statement from the International Liaison Committee on Resuscitation (American Heart Association, Australian and New Zealand Council on Resuscitation, European Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Asia, and the Resuscitation Council of Southern Africa); the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; and the Stroke Council. Circulation. 2008;118:2452–83. - PubMed
Publication types
MeSH terms
Grants and funding
- UL1 TR000433/TR/NCATS NIH HHS/United States
- R21 HD044955/HD/NICHD NIH HHS/United States
- R34 HD050531/HD/NICHD NIH HHS/United States
- P30 HD040677/HD/NICHD NIH HHS/United States
- U10 HD050096/HD/NICHD NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- K23 DK119463/DK/NIDDK NIH HHS/United States
- UL1 TR001417/TR/NCATS NIH HHS/United States
- UL1 RR024986/RR/NCRR NIH HHS/United States
- U01 HL094339/HL/NHLBI NIH HHS/United States
- U10 HD050012/HD/NICHD NIH HHS/United States
- R01 HL119542/HL/NHLBI NIH HHS/United States
- U10 HD049945/HD/NICHD NIH HHS/United States
- U54 HD087011/HD/NICHD NIH HHS/United States
- U10 HD049981/HD/NICHD NIH HHS/United States
- U01 HL094345/HL/NHLBI NIH HHS/United States
- U10 HD049983/HD/NICHD NIH HHS/United States
- R01 FD005092/FD/FDA HHS/United States
- U01 HD049934/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
