

Is hemiarch replacement adequate in acute type A aortic dissection repair in patients with arch branch vessel dissection without cerebral malperfusion?
- PMID: 33451835
- PMCID: PMC7935741
- DOI: 10.1016/j.jtcvs.2020.10.160
Is hemiarch replacement adequate in acute type A aortic dissection repair in patients with arch branch vessel dissection without cerebral malperfusion?
Abstract
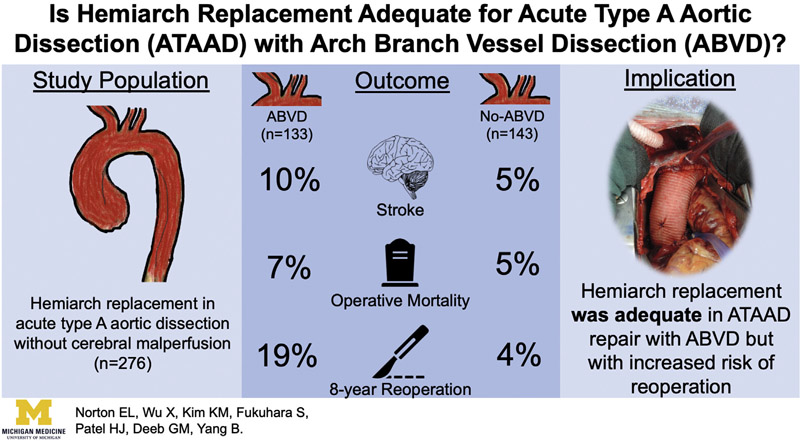
Objective: The study objective was to determine if hemiarch replacement is an adequate arch management strategy for patients with acute type A aortic dissection and arch branch vessel dissection but no cerebral malperfusion.
Methods: From January 2008 to August 2019, 479 patients underwent open acute type A aortic dissection repair. After excluding those with aggressive arch replacement (n = 168), cerebral malperfusion syndrome (n = 34), and indeterminable arch branch vessel dissection (n = 1), 276 patients with an acute type A aortic dissection without cerebral malperfusion syndrome who underwent hemiarch replacement comprised this study. Patients were then divided into those with arch branch vessel dissection (n = 133) and those with no arch branch vessel dissection (n = 143).
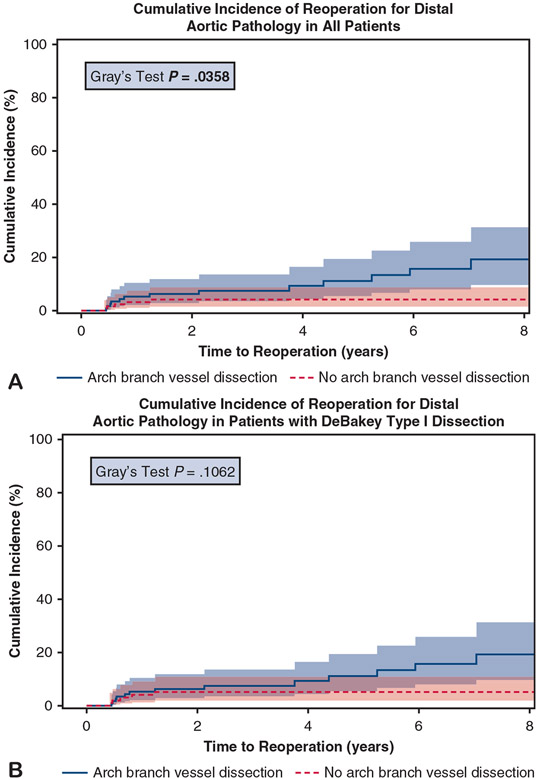
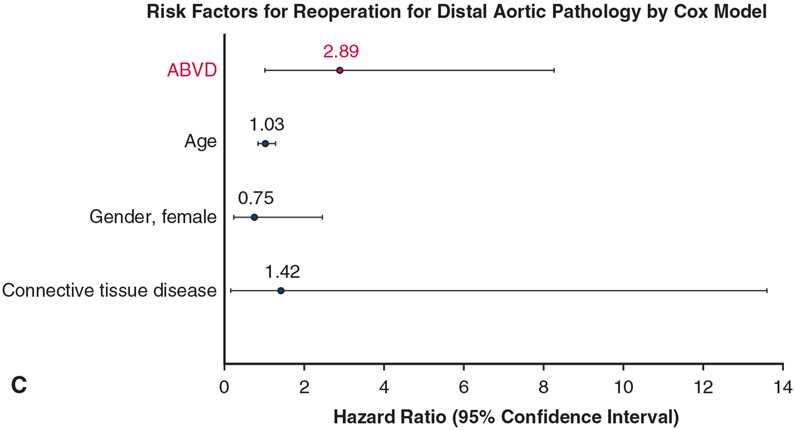
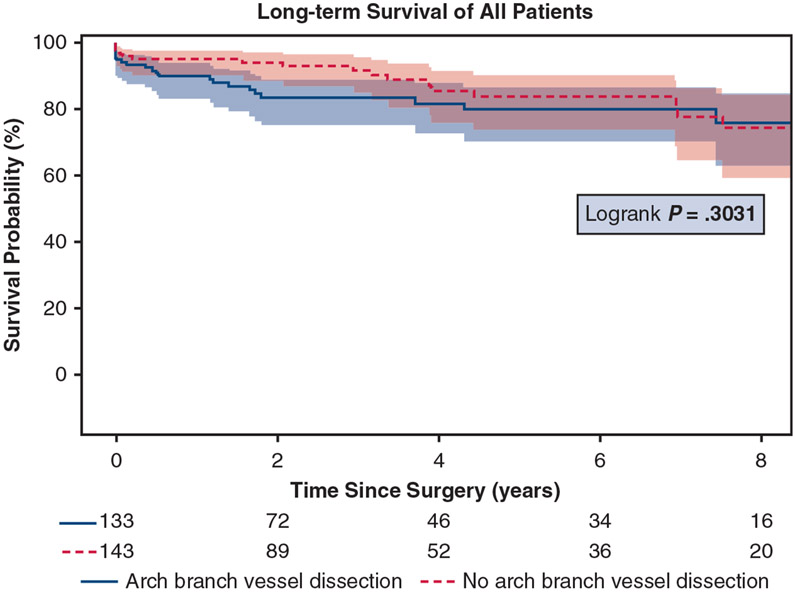
Results: The median age of the entire cohort was 62 years, with the arch branch vessel dissection group being younger (60 vs 62 years, P = .048). Both groups had similar aortic arch and descending thoracic aortic diameters, with significantly more DeBakey type I dissections (100% vs 80%) in the arch branch vessel dissection group. The arch branch vessel dissection group had more aortic root replacement (36% vs 27%, P = .0035) and longer aortic crossclamp times (153 vs 128 minutes, P = .007). Postoperative outcomes were similar between the arch branch vessel dissection and no arch branch vessel dissection groups, including stroke (10% vs 5%, P = .12) and operative morality (7% vs 5%, P = .51). The arch branch vessel dissection group had a significantly greater cumulative incidence of reoperation (8-year: 19% vs 4%, P = .04) with a hazard ratio of 2.89 (95% confidence interval, 1.01-8.27; P = .048), which was similar between groups among only DeBakey type I dissections (8-year: 19% vs 5%, P = .11). The 8-year survival was similar between the arch branch vessel dissection and no arch branch vessel dissection groups (76% vs 74%, P = .30).
Conclusions: Hemiarch replacement was adequate for patients with acute type A aortic dissection with arch branch vessel dissection without cerebral malperfusion syndrome, but carried a higher risk of late reoperation.
Keywords: acute aortic dissection; aortic arch management; arch branch vessel dissection.
Copyright © 2020 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest Statement
H.J.P. is a consultant for WL Gore and Associates, Edwards, and Medtronic, and these efforts are modest. All other authors reported no conflicts of interest.
The
Figures
Comment in
-
Commentary: Hemiarch replacement for acute type A dissection: Are we doing enough?J Thorac Cardiovasc Surg. 2021 Mar;161(3):888-889. doi: 10.1016/j.jtcvs.2020.11.039. Epub 2020 Nov 20. J Thorac Cardiovasc Surg. 2021. PMID: 33293070 No abstract available.
-
Commentary: Total arch or semiarch: That is the question.J Thorac Cardiovasc Surg. 2021 Mar;161(3):886-887. doi: 10.1016/j.jtcvs.2020.11.057. Epub 2020 Nov 23. J Thorac Cardiovasc Surg. 2021. PMID: 33339604 No abstract available.
-
Commentary: Don't forget the branches.J Thorac Cardiovasc Surg. 2021 Mar;161(3):885-886. doi: 10.1016/j.jtcvs.2020.11.084. Epub 2020 Nov 28. J Thorac Cardiovasc Surg. 2021. PMID: 33353750 No abstract available.
References
-
- Tsai TT, Trimarchi S, Nienaber CA. Acute aortic dissection: perspectives from the international registry of acute aortic dissection (IRAD). Eur J Vasc Endovasc Surg. 2009;37:149–59. - PubMed
-
- Chikwe J, Cavallaro P, Itagaki S, Seigerman M, Diluozzo G, Adams DH. National outcomes in acute aortic dissection: influence of surgeon and institutional volume on operative mortality. Ann Thorac Surg. 2013;95:1563–9. - PubMed
-
- Westaby S, Saito S, Katsumata T. Acute type A dissection: conservative methods provide consistently low mortality. Ann Thorac Surg. 2002;73:707–13. - PubMed
-
- Shiono M, Hata M, Sezai A, Niino T, Yagi S, Negishi N. Validity of a limited ascending and hemiarch replacement for acute type A aortic dissection. Ann Thorac Surg. 2006;82:1665–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
