

180-day readmission risk model for older adults with acute myocardial infarction: the SILVER-AMI study
- PMID: 33452007
- PMCID: PMC7813425
- DOI: 10.1136/openhrt-2020-001442
180-day readmission risk model for older adults with acute myocardial infarction: the SILVER-AMI study
Erratum in
-
Correction: 180-day readmission risk model for older adults with acute myocardial infarction: the SILVER-AMI study.Open Heart. 2021 Oct;8(2):1. doi: 10.1136/openhrt-2020-001442corr1. Open Heart. 2021. PMID: 34663752 Free PMC article. No abstract available.
Abstract
Objective: To develop a 180-day readmission risk model for older adults with acute myocardial infarction (AMI) that considered a broad range of clinical, demographic and age-related functional domains.
Methods: We used data from ComprehenSIVe Evaluation of Risk in Older Adults with AMI (SILVER-AMI), a prospective cohort study that enrolled participants aged ≥75 years with AMI from 94 US hospitals. Participants underwent an in-hospital assessment of functional impairments, including cognition, vision, hearing and mobility. Clinical variables previously shown to be associated with readmission risk were also evaluated. The outcome was 180-day readmission. From an initial list of 72 variables, we used backward selection and Bayesian model averaging to derive a risk model (N=2004) that was subsequently internally validated (N=1002).
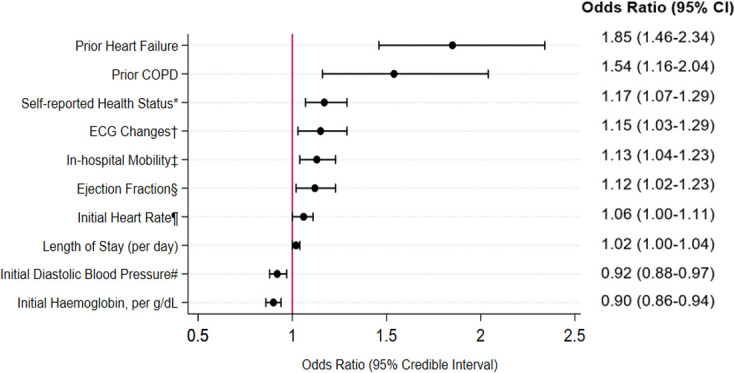
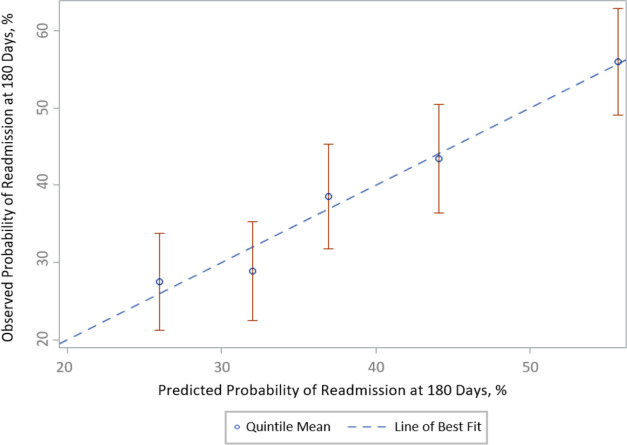
Results: Of the 3006 SILVER-AMI participants discharged alive, mean age was 81.5 years, 44.4% were women and 10.5% were non-white. Within 180 days, 1222 participants (40.7%) were readmitted. The final risk model included 10 variables: history of chronic obstructive pulmonary disease, history of heart failure, initial heart rate, first diastolic blood pressure, ischaemic ECG changes, initial haemoglobin, ejection fraction, length of stay, self-reported health status and functional mobility. Model discrimination was moderate (0.68 derivation cohort, 0.65 validation cohort), with good calibration. The predicted readmission rate (derivation cohort) was 23.0% in the lowest quintile and 65.4% in the highest quintile.
Conclusions: Over 40% of participants in our sample experienced hospital readmission within 180 days of AMI. Our final readmission risk model included a broad range of characteristics, including functional mobility and self-reported health status, neither of which have been previously considered in 180-day risk models.
Keywords: acute coronary syndrome; epidemiology; health care; outcome assessment.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: SIC receives funding for her work as a reviewer for the CVS Caremark Clinical Pharmacy Program for the state of Connecticut.
Figures
Similar articles
-
Development and Validation of a Risk Prediction Model for 1-Year Readmission Among Young Adults Hospitalized for Acute Myocardial Infarction.J Am Heart Assoc. 2021 Sep 21;10(18):e021047. doi: 10.1161/JAHA.121.021047. Epub 2021 Sep 13. J Am Heart Assoc. 2021. PMID: 34514837 Free PMC article.
-
Thirty-Day Readmission Risk Model for Older Adults Hospitalized With Acute Myocardial Infarction.Circ Cardiovasc Qual Outcomes. 2019 May;12(5):e005320. doi: 10.1161/CIRCOUTCOMES.118.005320. Circ Cardiovasc Qual Outcomes. 2019. PMID: 31010300 Free PMC article.
-
Predicting 6-Month Mortality for Older Adults Hospitalized With Acute Myocardial Infarction: A Cohort Study.Ann Intern Med. 2020 Jan 7;172(1):12-21. doi: 10.7326/M19-0974. Epub 2019 Dec 10. Ann Intern Med. 2020. PMID: 31816630 Free PMC article.
-
Acute Myocardial Infarction Readmission Risk Prediction Models: A Systematic Review of Model Performance.Circ Cardiovasc Qual Outcomes. 2018 Jan;11(1):e003885. doi: 10.1161/CIRCOUTCOMES.117.003885. Circ Cardiovasc Qual Outcomes. 2018. PMID: 29321135 Free PMC article.
-
The prevalence of 30-day readmission after acute myocardial infarction: A systematic review and meta-analysis.Clin Cardiol. 2019 Oct;42(10):889-898. doi: 10.1002/clc.23238. Epub 2019 Aug 12. Clin Cardiol. 2019. PMID: 31407368 Free PMC article.
Cited by
-
The performance of the Dutch Safety Management System frailty tool to predict the risk of readmission or mortality in older hospitalised cardiac patients.BMC Geriatr. 2021 May 8;21(1):299. doi: 10.1186/s12877-021-02243-5. BMC Geriatr. 2021. PMID: 33964888 Free PMC article.
-
Risk Prediction Models for Ischemic Cardiovascular Outcomes in Patients with Acute Coronary Syndrome.Rev Cardiovasc Med. 2023 Apr 13;24(4):106. doi: 10.31083/j.rcm2404106. eCollection 2023 Apr. Rev Cardiovasc Med. 2023. PMID: 39076282 Free PMC article. Review.
-
A Geriatric Approach to Percutaneous Coronary Interventions in Older Adults, Part II: A JACC: Advances Expert Panel.JACC Adv. 2023 Jul;2(5):100421. doi: 10.1016/j.jacadv.2023.100421. Epub 2023 Jul 28. JACC Adv. 2023. PMID: 37575202 Free PMC article.
-
Systematic Review and Critical Appraisal of Prediction Models for Readmission in Coronary Artery Disease Patients: Assessing Current Efficacy and Future Directions.Risk Manag Healthc Policy. 2024 Mar 12;17:549-557. doi: 10.2147/RMHP.S451436. eCollection 2024. Risk Manag Healthc Policy. 2024. PMID: 38496372 Free PMC article. Review.
-
Development and Validation of a Risk Prediction Model for 1-Year Readmission Among Young Adults Hospitalized for Acute Myocardial Infarction.J Am Heart Assoc. 2021 Sep 21;10(18):e021047. doi: 10.1161/JAHA.121.021047. Epub 2021 Sep 13. J Am Heart Assoc. 2021. PMID: 34514837 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical