

The effectiveness of training strategies to improve healthcare provider practices in low-income and middle-income countries
- PMID: 33452138
- PMCID: PMC7813291
- DOI: 10.1136/bmjgh-2020-003229
The effectiveness of training strategies to improve healthcare provider practices in low-income and middle-income countries
Abstract
Introduction: In low/middle-income countries (LMICs), training is often used to improve healthcare provider (HCP) performance. However, important questions remain about how well training works and the best ways to design training strategies. The objective of this study is to characterise the effectiveness of training strategies to improve HCP practices in LMICs and identify attributes associated with training effectiveness.
Methods: We performed a secondary analysis of data from a systematic review on improving HCP performance. The review included controlled trials and interrupted time series, and outcomes measuring HCP practices (eg, percentage of patients correctly treated). Distributions of effect sizes (defined as percentage-point (%-point) changes) were described for each training strategy. To identify effective training attributes, we examined studies that directly compared training approaches and performed random-effects linear regression modelling.
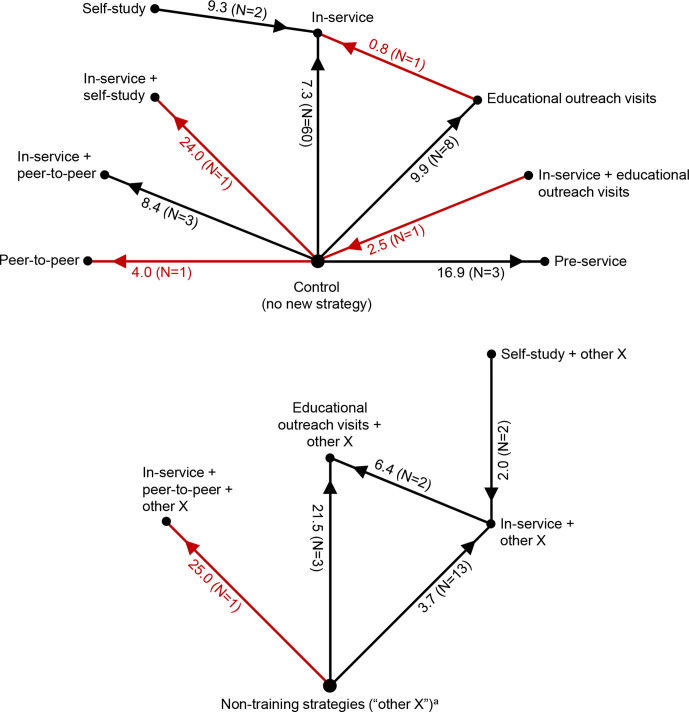
Results: We analysed data from 199 studies from 51 countries. For outcomes expressed as percentages, educational outreach visits (median effect size when compared with controls: 9.9 %-points; IQR: 4.3-20.6) tended to be somewhat more effective than in-service training (median: 7.3 %-points; IQR: 3.6-17.4), which seemed more effective than peer-to-peer training (4.0 %-points) and self-study (by 2.0-9.3 %-points). Mean effectiveness was greater (by 6.0-10.4 %-points) for training that incorporated clinical practice and training at HCPs' work site. Attributes with little or no effect were: training with computers, interactive methods or over multiple sessions; training duration; number of educational methods; distance training; trainers with pedagogical training and topic complexity. For lay HCPs, in-service training had no measurable effect. Evidence quality for all findings was low.
Conclusions: Although additional research is needed, by characterising the effectiveness of training strategies and identifying attributes of effective training, decision-makers in LMICs can improve how these strategies are selected and implemented.
Keywords: health services research.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- World Health Organization Ninth programme report 1992–1993. Geneva: Programme for Control of Diarrhoeal Diseases, World Health Organization, 1994.
-
- President’s Malaria Initiative Fiscal year 2017 malaria operational plans. Available: https://www.pmi.gov/resource-library/mops/fy-2017 [Accessed 11 Feb 2019].
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous