

PMCA4 inhibition does not affect cardiac remodelling following myocardial infarction, but may reduce susceptibility to arrhythmia
- PMID: 33452399
- PMCID: PMC7810749
- DOI: 10.1038/s41598-021-81170-2
PMCA4 inhibition does not affect cardiac remodelling following myocardial infarction, but may reduce susceptibility to arrhythmia
Abstract
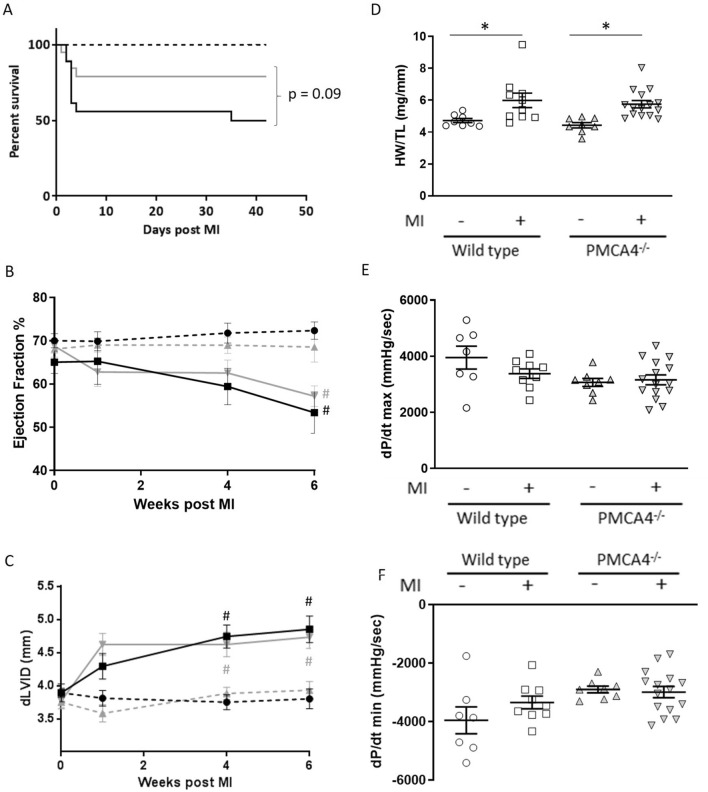
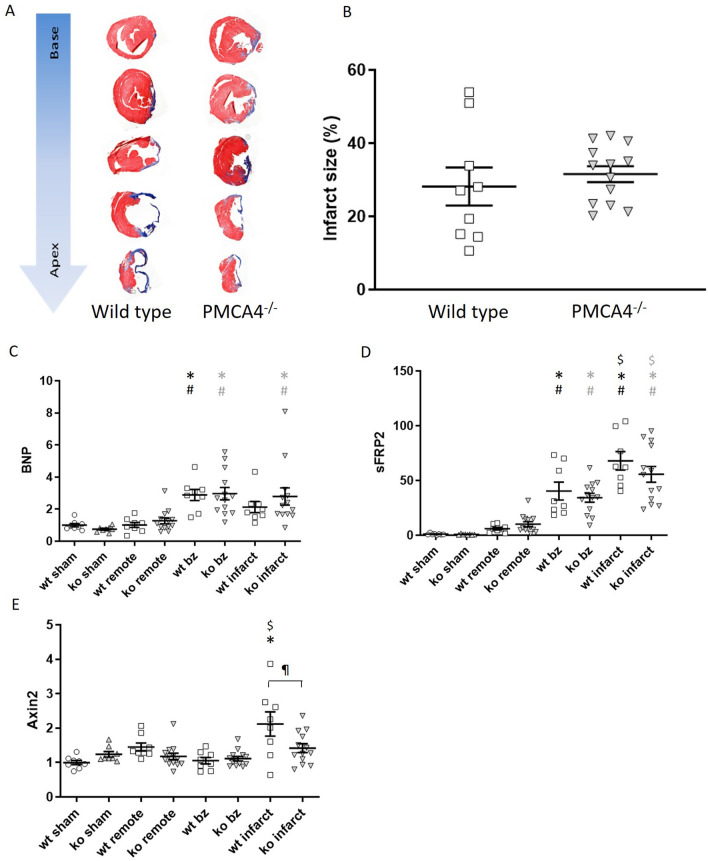
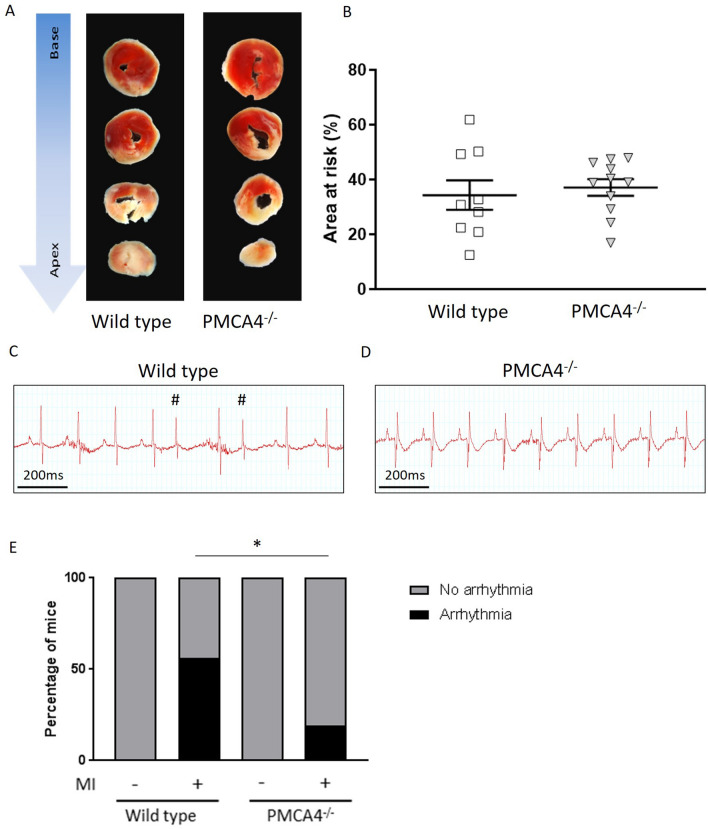
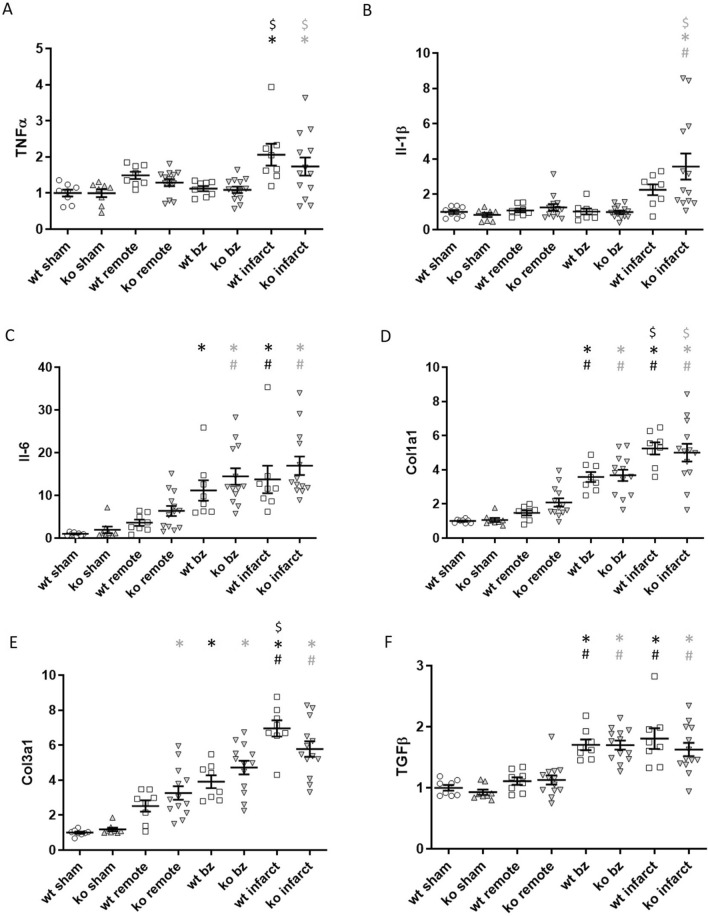
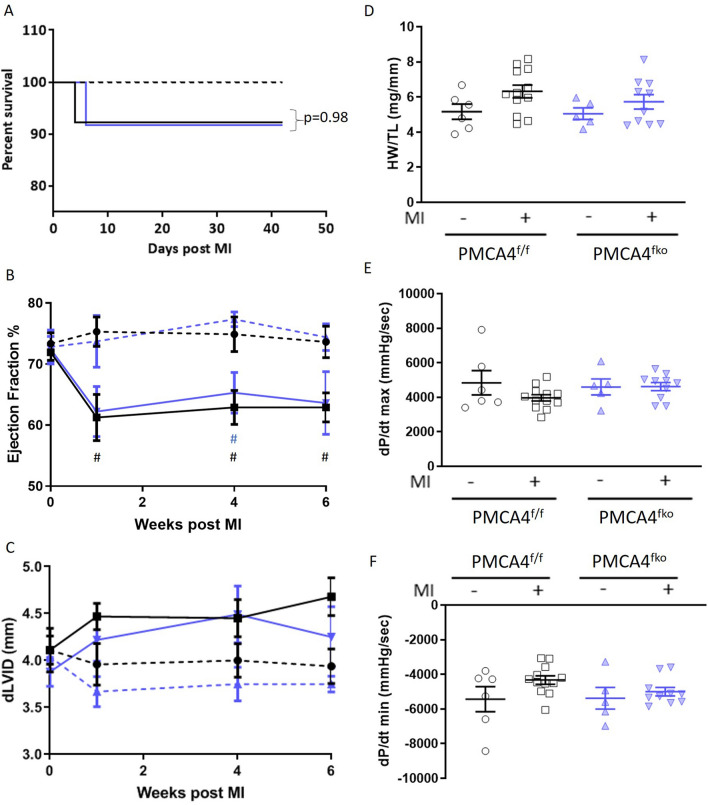
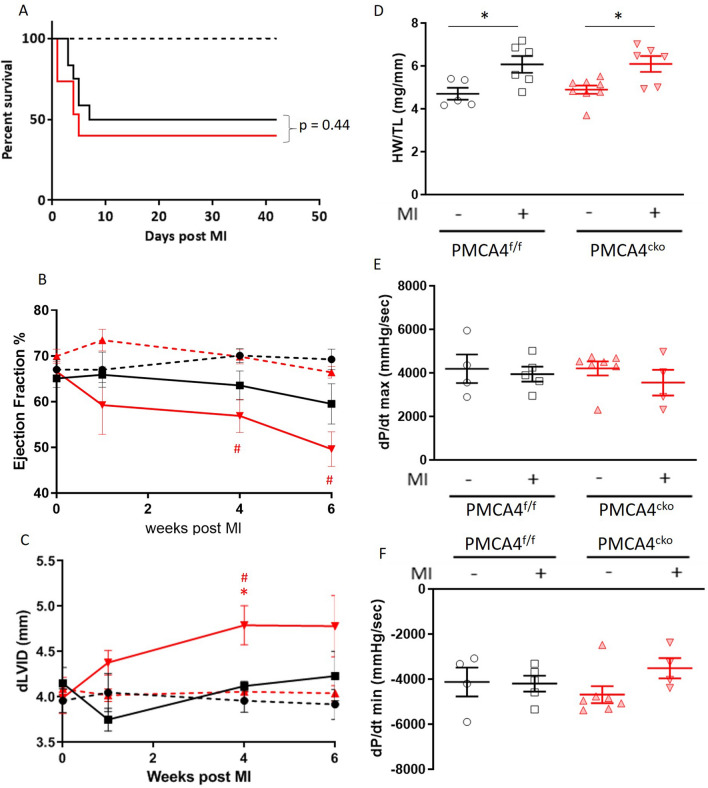
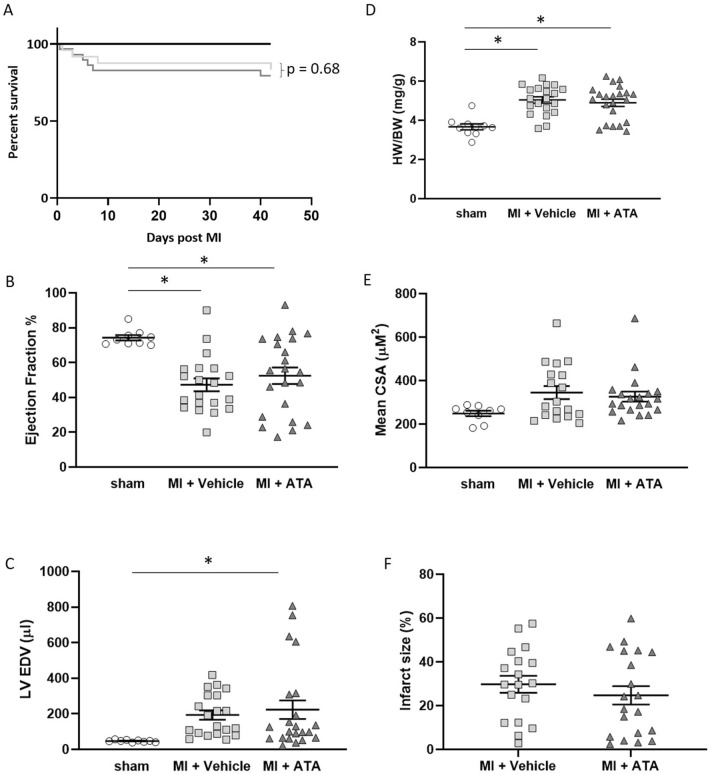
Ischaemic heart disease is the world's leading cause of mortality. Survival rates from acute myocardial infarction (MI) have improved in recent years; however, this has led to an increase in the prevalence of heart failure (HF) due to chronic remodelling of the infarcted myocardium, for which treatment options remain poor. We have previously shown that inhibition of isoform 4 of the plasma membrane calcium ATPase (PMCA4) prevents chronic remodelling and HF development during pressure overload, through fibroblast mediated Wnt signalling modulation. Given that Wnt signalling also plays a prominent role during remodelling of the infarcted heart, this study investigated the effect of genetic and functional loss of PMCA4 on cardiac outcomes following MI. Neither genetic deletion nor pharmacological inhibition of PMCA4 affected chronic remodelling of the post-MI myocardium. This was the case when PMCA4 was deleted globally, or specifically from cardiomyocytes or fibroblasts. PMCA4-ablated hearts were however less prone to acute arrhythmic events, which may offer a slight survival benefit. Overall, this study demonstrates that PMCA4 inhibition does not affect chronic outcomes following MI.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Wilkins, E. et al. European Cardiovascular Disease Statistics 2017. (2017). - PubMed
-
- Townsend N, Bhatnagar P, Wilkins E, Wickramasinghe K. Cardiovascular Disease Statistics 2015. London: British Heart Foundation; 2015.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
