

Surfactant lung delivery with LISA and InSurE in adult rabbits with respiratory distress
- PMID: 33452472
- PMCID: PMC7809896
- DOI: 10.1038/s41390-020-01324-2
Surfactant lung delivery with LISA and InSurE in adult rabbits with respiratory distress
Abstract
Background: In preterm infants, InSurE (Intubation-Surfactant-Extubation) and LISA (less invasive surfactant administration) techniques allow for exogenous surfactant administration while reducing lung injury associated with mechanical ventilation. We compared the acute pulmonary response and lung deposition of surfactant by LISA and InSurE in surfactant-depleted adult rabbits.
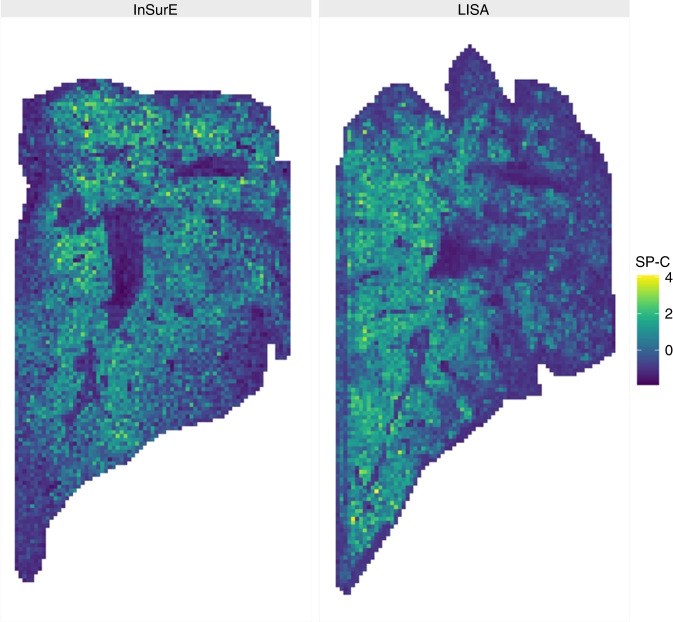
Methods: Twenty-six spontaneously breathing surfactant-depleted adult rabbits (6-7 weeks old) with moderate RDS and managed with nasal continuous positive airway pressure were randomized to 3 groups: (1) 200 mg/kg of surfactant by InSurE; (2) 200 mg/kg of surfactant by LISA; (3) no surfactant treatment (Control). Gas exchange and lung mechanics were monitored for 180 min. After that, surfactant lung deposition and distribution were evaluated monitoring disaturated-phosphatidylcholine (DSPC) and surfactant protein C (SP-C), respectively.
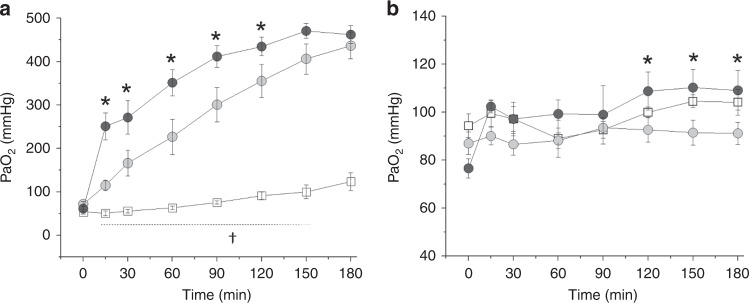
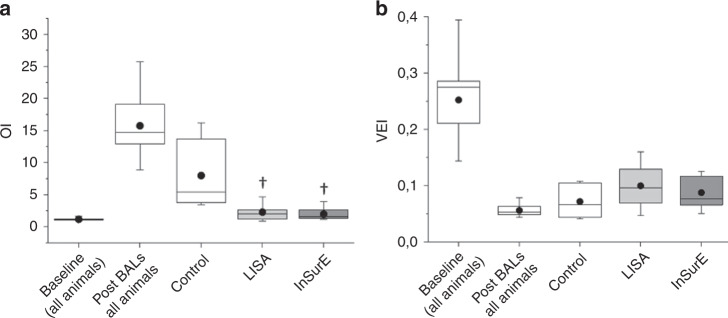
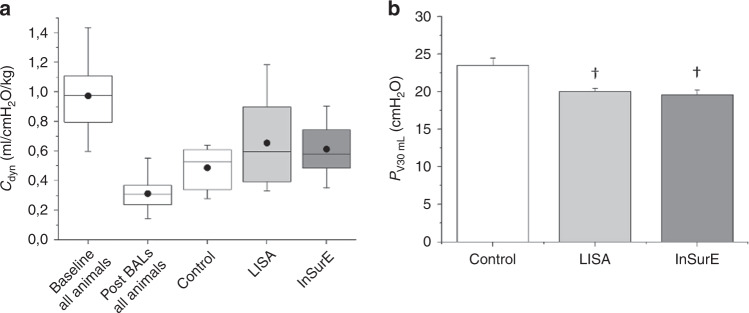
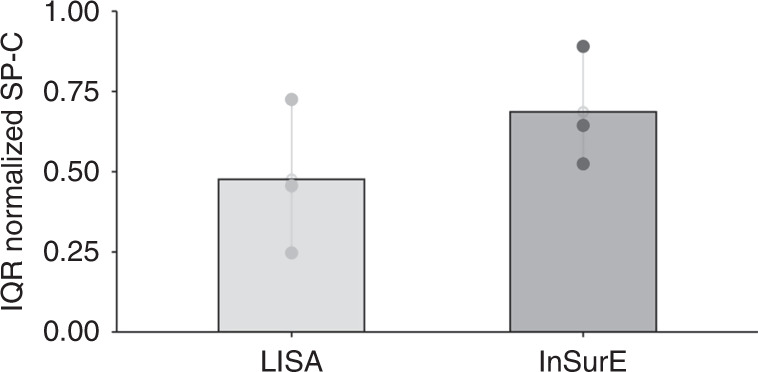
Results: No signs of recovery were found in the untreated animals. After InSurE, oxygenation improved more rapidly compared to LISA. However, at 180' LISA and InSurE showed comparable outcomes in terms of gas exchange, ventilation parameters, and lung mechanics. Neither DSPC in the alveolar pool nor SP-C signal distributions in a frontal lung section were significantly different between InSurE and LISA groups.
Conclusions: In an acute setting, LISA demonstrated efficacy and surfactant lung delivery similar to that of InSurE in surfactant-depleted adult rabbits.
Impact: Although LISA technique is gaining popularity, there are still several questions to address. This is the first study comparing LISA and InSurE in terms of gas exchange, ventilation parameters, and lung mechanics as well as surfactant deposition and distribution. In our animal study, three hours post-treatment, LISA method seems to be as effective as InSurE and showed similar surfactant lung delivery. Our findings provide some clarifications on a fair comparison between LISA and InSurE techniques, particularly in terms of surfactant delivery. They should reassure some of the concerns raised by the clinical community on LISA adoption in neonatal units.
© 2021. The Author(s), under exclusive licence to the International Pediatric Research Foundation, Inc.
Conflict of interest statement
F.R., F.S., C. Casiraghi, C. Catozzi, and L.T. are Chiesi Farmaceutici SpA employees. X.M. acts as Chiesi Farmaceutici SpA scientific consultant.
Figures

References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
