

Review
doi: 10.1245/s10434-020-09566-4.
Epub 2021 Jan 15.
The Landmark Series: Management of Small Bowel Neuroendocrine Tumors
Affiliations
- PMID: 33452604
- PMCID: PMC8604156
- DOI: 10.1245/s10434-020-09566-4
Item in Clipboard
Review
The Landmark Series: Management of Small Bowel Neuroendocrine Tumors
Ann Surg Oncol.
2021 May.
Abstract
Surgical resection is the foundation for treatment of small bowel neuroendocrine tumors (SBNETs). Guidelines for surgical management of SBNETs rely on retrospective data, which suggest that primary tumor resection and cytoreduction improve symptoms, prevent future complications, and lengthen survival. In advanced NETs, improvement in progression-free survival has been reported in large, randomized, controlled trials of various medical treatments, including somatostatin analogues, targeted therapy, and peptide receptor radionuclide therapy. This review discusses important studies influencing the management of SBNETs and the limitations of current evidence regarding surgical interventions for SBNETs.
Figures
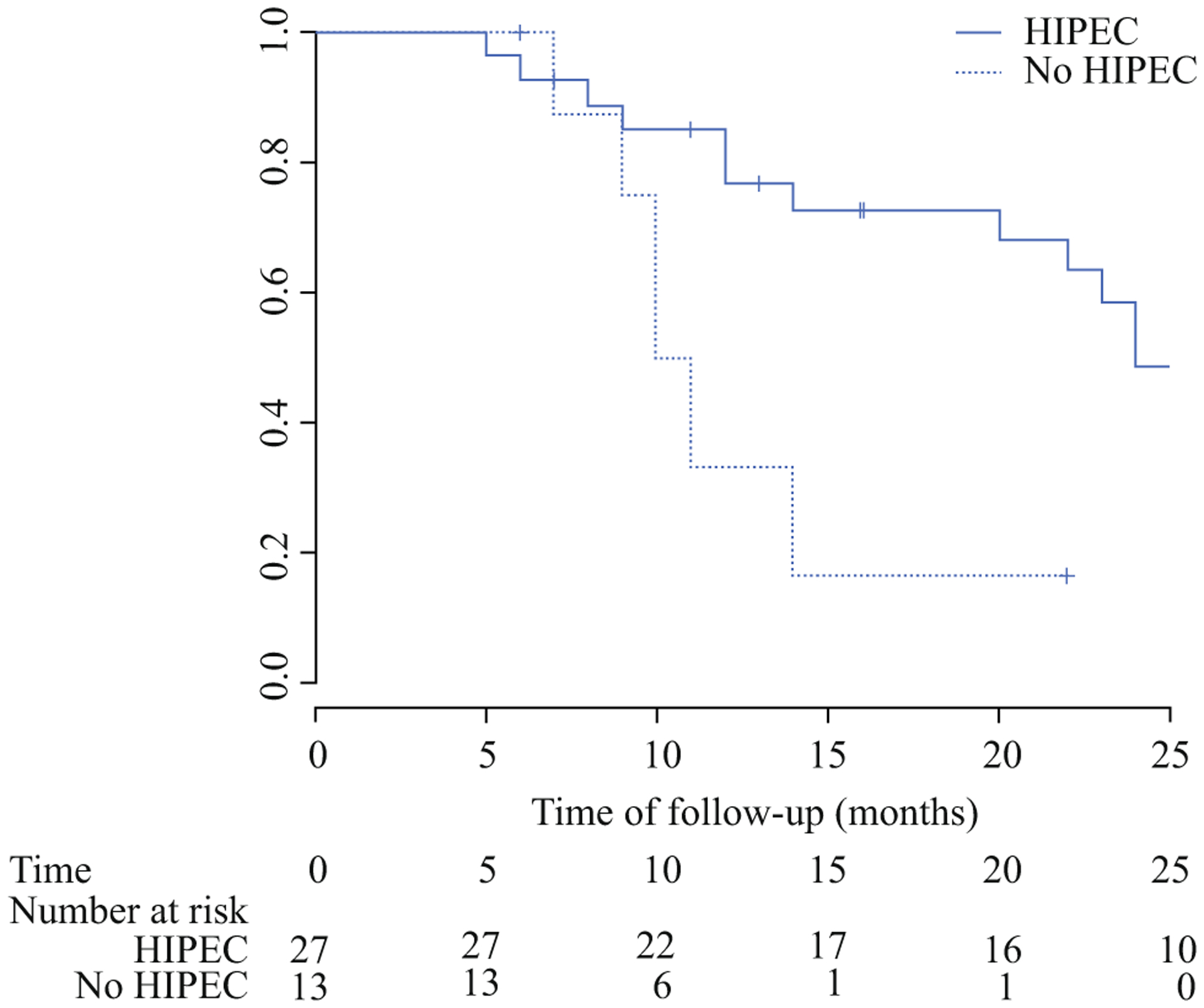
Disease-free survival of patients with NET peritoneal carcinomatosis undergoing cytoreduction and HIPEC versus cytoreduction alone in Elias et al. Disease-free survival (DFS) was longer in the HIPEC group compared with the non-HIPEC group (2-year DFS 49% vs. 16.7%, P = 0.018), although there were no differences in OS, peritoneal recurrence rates, or liver recurrence rates. HIPEC is not currently recommended for NET treatment. HIPEC Heated intraperitoneal chemotherapy, NET Neuroendocrine tumor, OS Overall survival
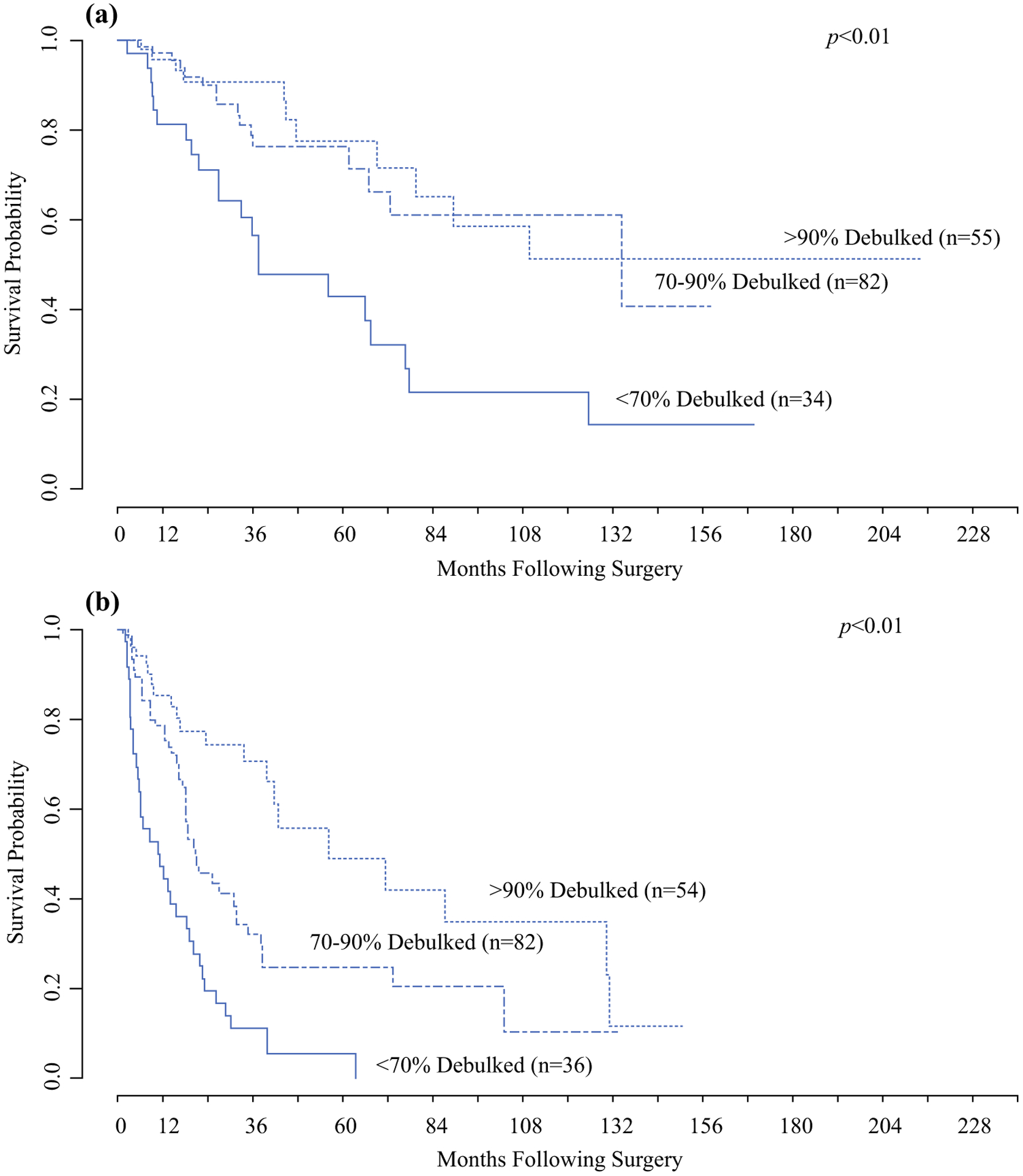
Kaplan–Meier curves of a OS and b PFS in patients with small bowel (SBNETs) or pancreatic (PNETs) neuroendocrine tumors who underwent hepatic cytoreduction in Scott et al. Patients with cytoreduction of at least 70% of their hepatic tumor burden had improved OS and PFS compared with patients with < 70% cytoreduction. OS Overall survival, PFS Progression-free survival
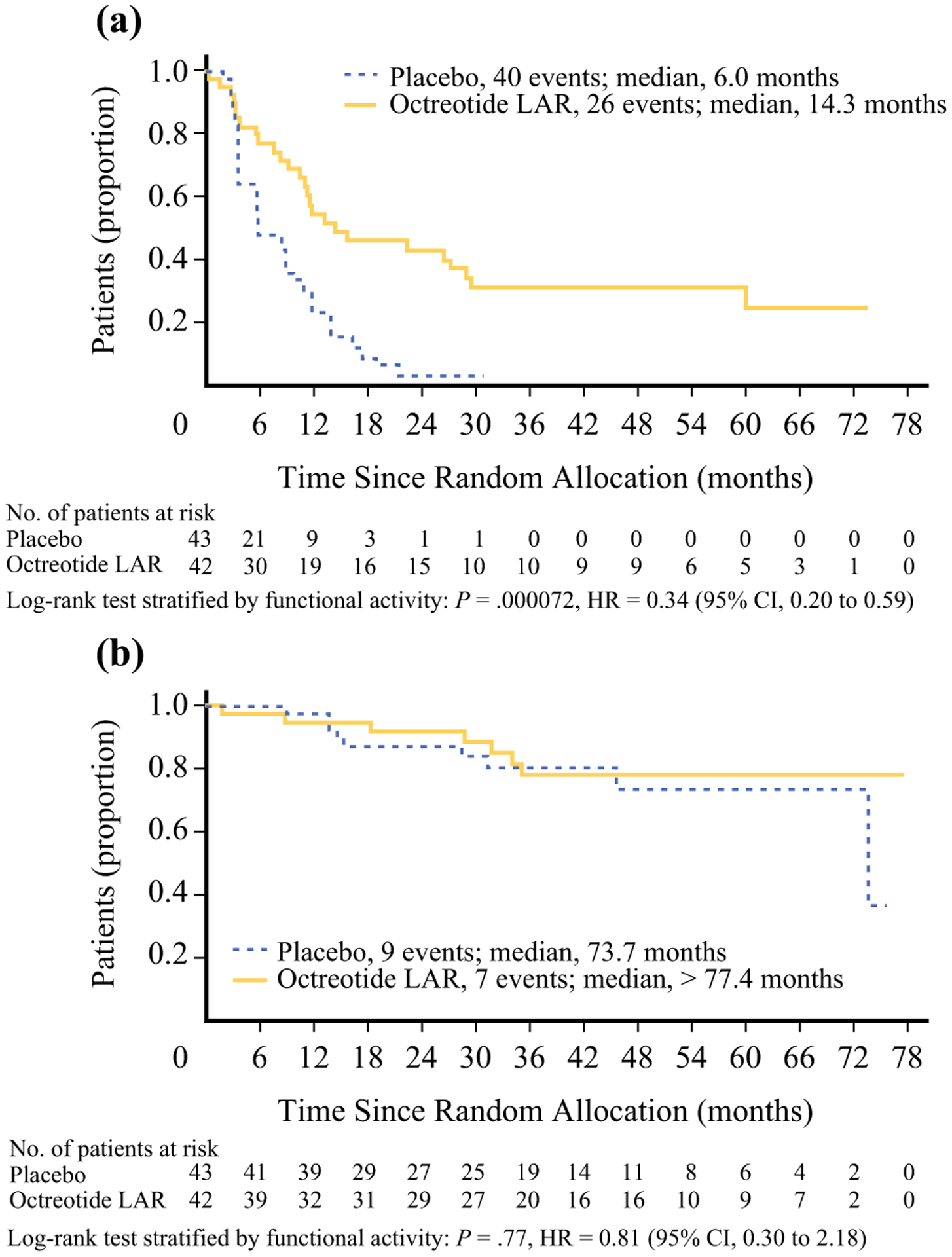
Survival outcomes from the PROMID trial. Kaplan–Meier analysis of a PFS and b OS in patients with advanced midgut NETs receiving octreotide long-acting repeatable (LAR) or placebo. The octreotide LAR group had longer PFS (14.3 vs. 5 months; HR 0.34, P = 0.000072). The two groups had similar OS, although the majority of patients in the placebo group (38/43) received octreotide upon progression. HR Hazard ratio, NET Neuroendocrine tumor, OS Overall survival, PFS Progression-free survival
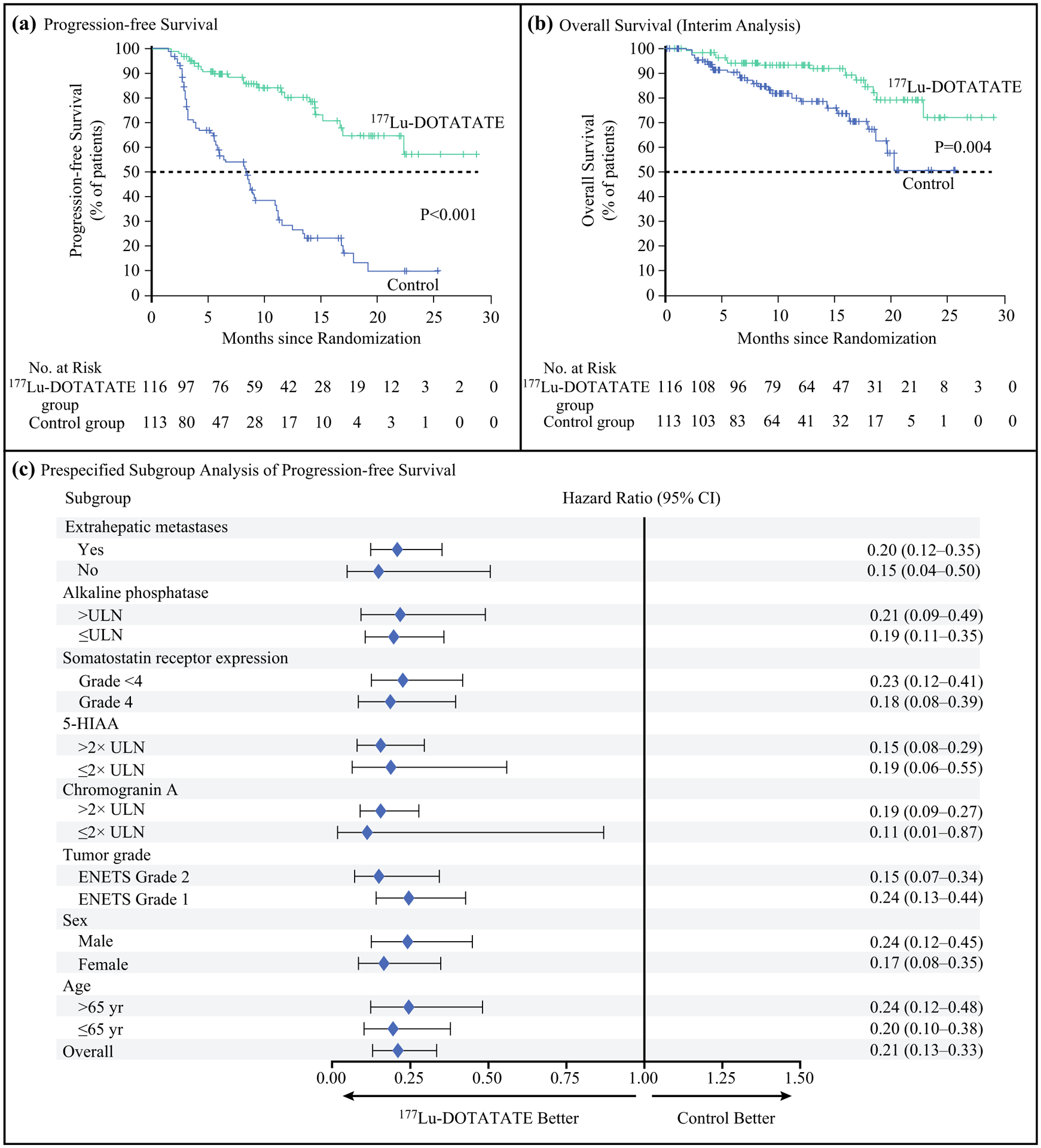
Survival outcomes from the NETTER-1 trial. Kaplan–Meier analyses of a PFS and b OS comparing patients with advanced midgut NETs who received 177Lu-Dotatate PRRT and octreotide LAR (30 mg/28 days) or high-dose octreotide LAR (60 mg/28 days). The 177Lu-Dotatate group had longer PFS (median not reached vs. 8.4 months; HR 0.21, P < 0.001). The hazard ratio for death was 0.4 (P = 0.004) in the 177Lu-Dotatate group, but data were not mature enough to determine median OS. c Effect of 177Lu-Dotatate treatment on PFS in prespecified subgroups. HR Hazard ratio, LAR Long-acting repeatable, NET Neuroendocrine tumor, OS Overall survival, PFS Progression-free survival, ULN Upper limit of normal range
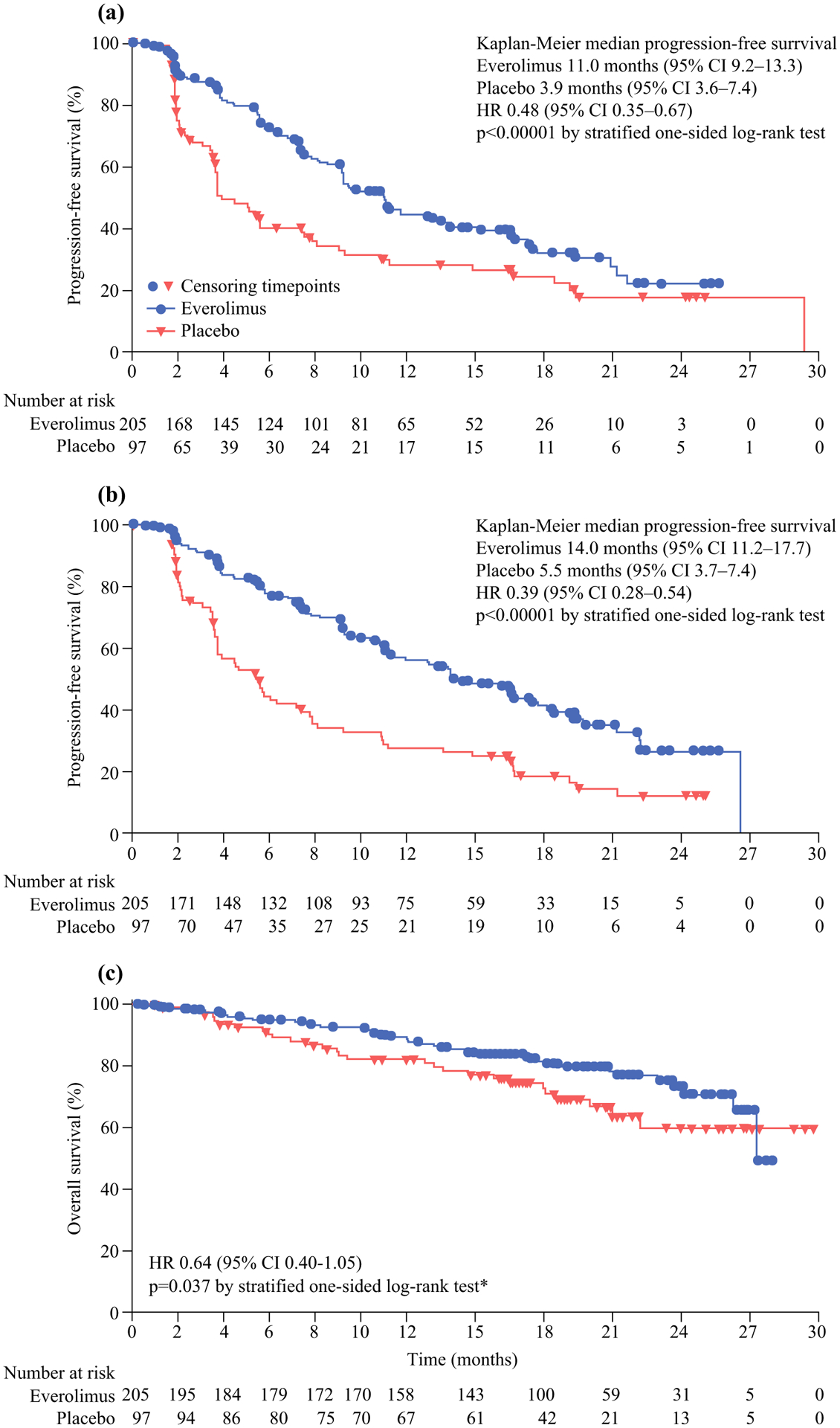
Survival outcomes from the RADIANT-4 trial comparing patients with advanced lung or GEP NETs who received everolimus or placebo. Kaplan–Meier curves of a PFS based on central radiology review, b PFS as determined by local investigators, and c OS. The everolimus group had improved PFS (median PFS 11.0 vs. 3.9 months; HR 0.48, P < 0.001). The difference in OS was not statistically significant based on the boundary for significance of 0.0002. GEP NET Gastroenteropancreatic neuroendocrine tumor, OS Overall survival, PFS Progression-free survival
References
-
- Moertel CG, Sauer WG, Dockerty MB, Baggenstoss AH. Life history of the carcinoid tumor of the small intestine. Cancer. 1961;14:901–12. - PubMed
-
- Kuiper DH, Gracie WA Jr., Pollard HM. Twenty years of gastrointestinal carcinoids. Cancer. 1970;25(6):1424–30. - PubMed
-
- Berge T, Linell F. Carcinoid tumours: frequency in a defined population during a 12-year-period. Acta Pathol Microbiol Scand A Pathol. 1976;84(4):322–30. - PubMed
-
- Burke AP, Thomas RM, Elsayed AM, Sobin LH. Carcinoids of the jejunum and ileum: an immunohistochemical and clinicopathologic study of 167 cases. Cancer. 1997;79(6):1086–93. - PubMed
-
- Wang SC, Parekh JR, Zuraek MB, et al. Identification of unknown primary tumors in patients with neuroendocrine liver metastases. Arch Surg. 2010;145(3):276–80. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
