

Black-White disparities in maternal in-hospital mortality according to teaching and Black-serving hospital status
- PMID: 33453183
- PMCID: PMC8254791
- DOI: 10.1016/j.ajog.2021.01.004
Black-White disparities in maternal in-hospital mortality according to teaching and Black-serving hospital status
Abstract
Background: Maternal mortality is higher among Black than White people in the United States. Whether Black-White disparities in maternal in-hospital mortality during the delivery hospitalization vary across hospital types (Black-serving vs nonBlack-serving and teaching vs nonteaching) and whether overall maternal mortality differs across hospital types is not known.
Objective: The aims of this study were to determine whether risk-adjusted Black-White disparities in maternal mortality during the delivery hospitalization vary by hospital types (this is analysis of disparities in mortality within hospital types) and compare risk-adjusted in-hospital maternal mortality among Black-serving and nonBlack-serving teaching and nonteaching hospitals regardless of race (this is an analysis of overall mortality across hospital types).
Study design: We performed a population-based, retrospective cohort study of 5,679,044 deliveries among Black (14.2%) and White patients (85.8%) in 3 states (California, Missouri, and Pennsylvania) from 1995 to 2009. A hospital discharge disposition of "death" defined maternal in-hospital mortality. Black-serving hospitals had at least 7% Black obstetrical patients (top quartile). We performed risk adjustment by calculating expected death rates using predictions from logistic regression models incorporating sociodemographics, rurality, comorbidities, multiple gestations, gestational age at delivery, year, state, and mode of delivery. We calculated risk-adjusted risk ratios of mortality by comparing observed-to-expected ratios among Black and White patients within hospital types and then examined mortality across hospital types, regardless of patient race. We quantified the proportion of Black-White disparities in mortality attributable to delivering in Black-serving hospitals using causal mediation analysis.
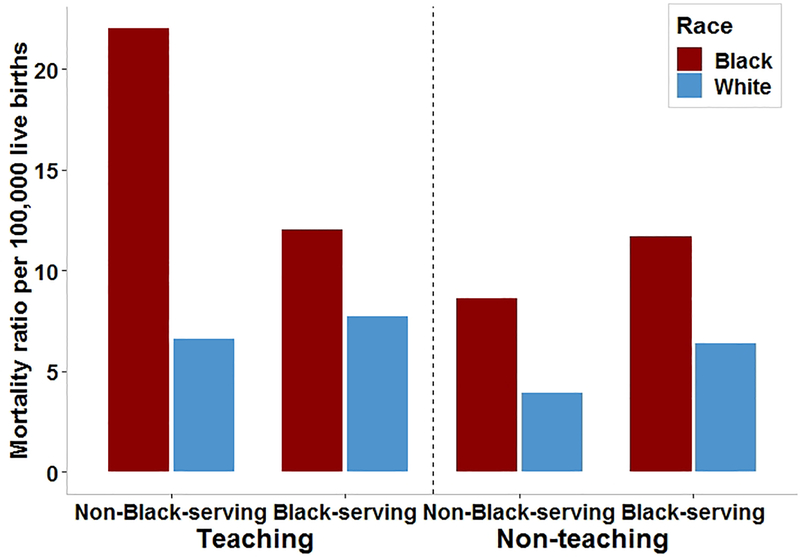
Results: There were 330 maternal deaths among 5,679,044 patients (5.8 per 100,000). Black patients died more often (11.5 per 100,000) than White patients (4.8 per 100,000) (relative risk, 2.38; 95% confidence interval, 1.89-2.98). Examination of Black-White disparities revealed that after risk adjustment, Black patients had significantly greater risk of death (adjusted relative risk, 1.44; 95% confidence interval, 1.17-1.79) and that the disparity was similar within each of the hospital types. Comparison of mortality, regardless of race, across hospital types revealed that among teaching hospitals, mortality was similar in Black-serving and nonBlack-serving hospitals. However, among nonteaching hospitals, mortality was significantly higher in Black-serving vs nonBlack-serving hospitals (adjusted relative risk, 1.47; 95% confidence interval, 1.15-1.87). Notably, 53% of Black patients delivered in nonteaching, Black-serving hospitals compared with just 19% of White patients. Among nonteaching hospitals, 47% of Black-White disparities in maternal in-hospital mortality were attributable to delivering at Black-serving hospitals.
Conclusion: Maternal in-hospital mortality during the delivery hospitalization among Black patients is more than double that of White patients. Our data suggest this disparity is caused by excess mortality among Black patients within each hospital type, in addition to excess mortality in nonteaching, Black-serving hospitals where most Black patients deliver. Addressing downstream effects of racism to achieve equity in maternal in-hospital mortality will require transparent reporting of quality metrics by race to reduce differential care and outcomes within hospital types, improvements in care delivery at Black-serving hospitals, overcoming barriers to accessing high-quality care among Black patients, and eventually desegregation of healthcare.
Keywords: cohort study; health equity; health services; inpatient mortality; maternal morbidity; maternal mortality; population study; pregnancy; racial disparities; racism.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Centers for Disease Control and Prevention. National Center for Health Statistics. Maternal mortality, 2020.
-
- Krieger N, Smith K, Naishadham D, Hartman C, Barbeau EM. Experiences of discrimination: validity and reliability of a self-report measure for population health research on racism and health. Soc Sci Med 2005;61:1576–96. - PubMed
-
- Boyd RW, Lindo EG, Weeks LD, MclemorE MR. On Racism: A New Standard For Publishing On Racial Health Inequities Health Affairs Blog, 2020. https://www.healthaffairs.org/do/10.1377/hblog20200630.939347/full/. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
