

Clinically applicable approach for predicting mechanical ventilation in patients with COVID-19
- PMID: 33454051
- PMCID: PMC7833820
- DOI: 10.1016/j.bja.2020.11.034
Clinically applicable approach for predicting mechanical ventilation in patients with COVID-19
Abstract
Background: Patients with coronavirus disease 2019 (COVID-19) requiring mechanical ventilation have high mortality and resource utilisation. The ability to predict which patients may require mechanical ventilation allows increased acuity of care and targeted interventions to potentially mitigate deterioration.
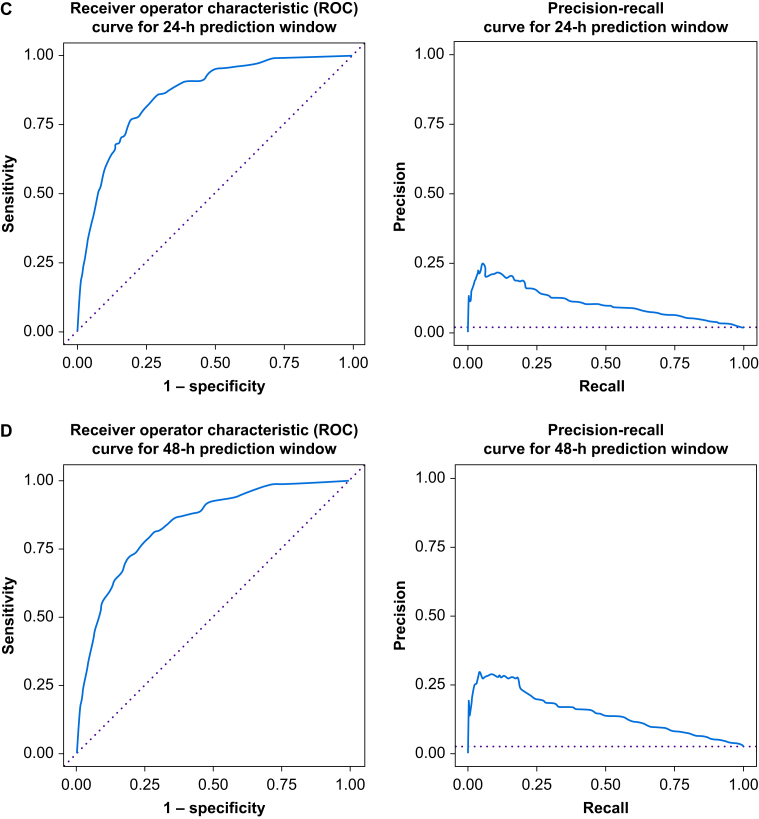
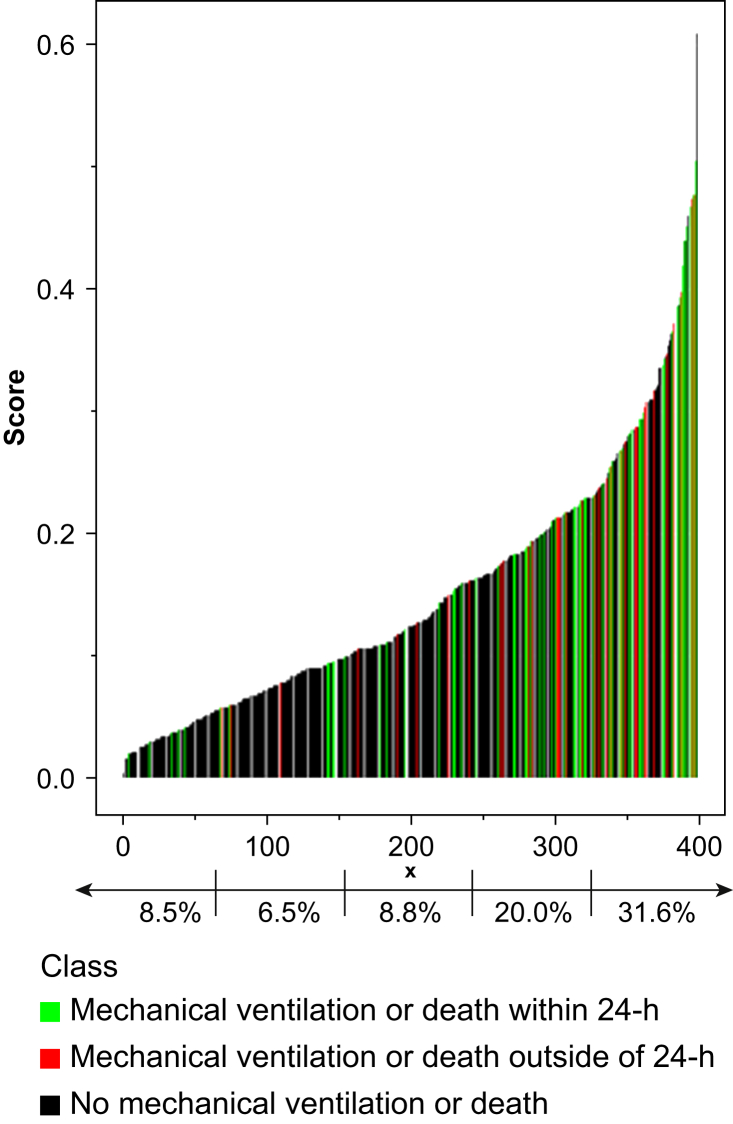
Methods: We included hospitalised patients with COVID-19 in this single-centre retrospective observational study. Our primary outcome was mechanical ventilation or death within 24 h. As clinical decompensation is more recognisable, but less modifiable, as the prediction window shrinks, we also assessed 4, 8, and 48 h prediction windows. Model features included demographic information, laboratory results, comorbidities, medication administration, and vital signs. We created a Random Forest model, and assessed performance using 10-fold cross-validation. The model was compared with models derived from generalised estimating equations using discrimination.
Results: Ninety-three (23%) of 398 patients required mechanical ventilation or died within 14 days of admission. The Random Forest model predicted pending mechanical ventilation with good discrimination (C-statistic=0.858; 95% confidence interval, 0.841-0.874), which is comparable with the discrimination of the generalised estimating equation regression. Vitals sign data including SpO2/FiO2 ratio (Random Forest Feature Importance Z-score=8.56), ventilatory frequency (5.97), and heart rate (5.87) had the highest predictive utility. In our highest-risk cohort, the number of patients needed to identify a single new case was 3.2, and for our second quintile it was 5.0.
Conclusion: Machine learning techniques can be leveraged to improve the ability to predict which patients with COVID-19 are likely to require mechanical ventilation, identifying unrecognised bellwethers and providing insight into the constellation of accompanying signs of respiratory failure in COVID-19.
Keywords: COVID-19; critical care medicine; machine learning; mechanical ventilation; predictive models; respiratory failure; respiratory insufficiency.
Copyright © 2020 British Journal of Anaesthesia. Published by Elsevier Ltd. All rights reserved.
Figures

References
-
- World Health Organization . 2020. Naming the coronavirus disease (COVID-19) and the virus that causes it.https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technica... Available from: accessed 23 April 2020.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
