

Practice patterns for postoperative radiation therapy in patients with metastases to the long bones: a survey of the Japanese Radiation Oncology Study Group
- PMID: 33454759
- PMCID: PMC7948830
- DOI: 10.1093/jrr/rraa133
Practice patterns for postoperative radiation therapy in patients with metastases to the long bones: a survey of the Japanese Radiation Oncology Study Group
Abstract
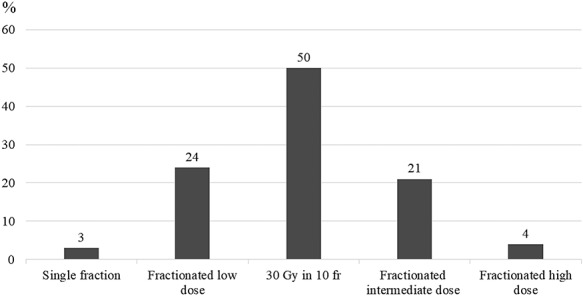
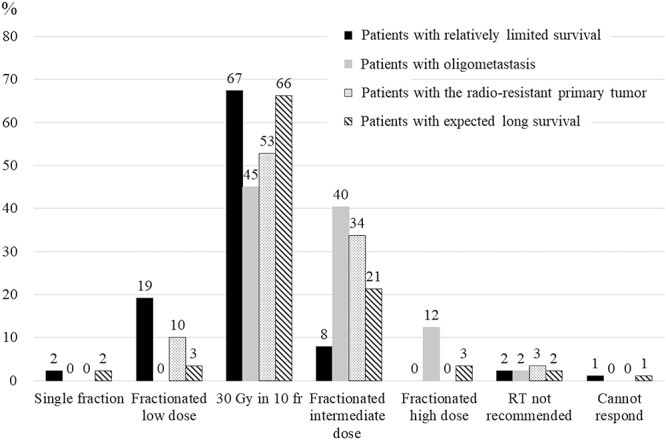
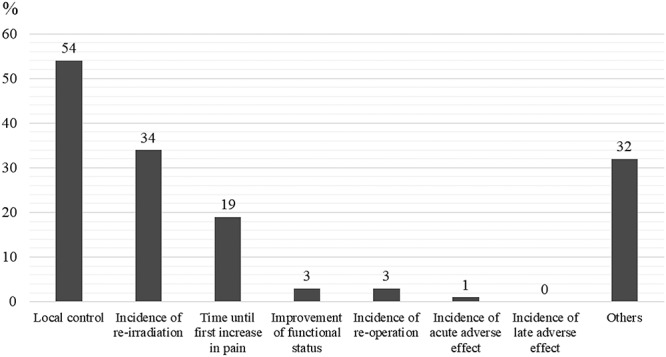
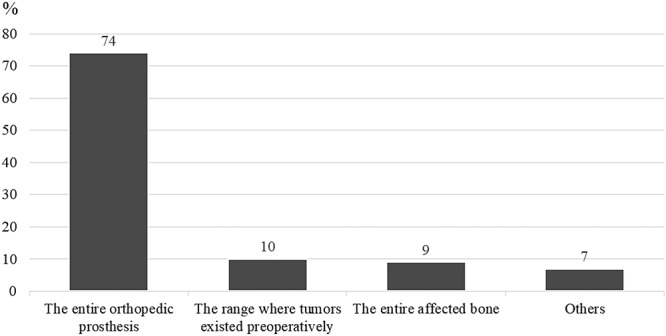
Evidence regarding postoperative radiation therapy (PORT) for metastases to the long bones is lacking. Characterizing the current practice patterns and identifying factors that influence dose-fractionation schedules are essential for future clinical trials. An internet-based survey of the palliative RT subgroup of the Japanese Radiation Oncology Study Group was performed in 2017 to collect data regarding PORT prescription practices and dose-fractionation schedules. Responders were also asked to recommend dose-fractionation schedules for four hypothetical cases that involved a patient with impending pathological fractures and one of four clinical features (poor prognosis, solitary metastasis, radio-resistant primary tumor or expected long-term survival). Responders were asked to indicate their preferred irradiation fields and the reasons for the dose fractionation schedule they chose. Responses were obtained from 89 radiation oncologists (67 institutions and 151 RT plans) who used 22 dose-fractionation schedules, with the most commonly used and recommended schedule being 30 Gy in 10 fractions. Local control was the most common reason for preferring longer-course RT. High-dose fractionated schedules were preferred for oligometastasis, and low-dose regimens were preferred for patients with a poor prognosis; however, single-fraction RT was not preferred. Most respondents recommended targeting the entire orthopedic prosthesis. These results indicated that PORT using 30 Gy in 10 fractions to the entire orthopedic prosthesis is preferred in current Japanese practice and that single-fraction RT was not preferred. Oligometastasis and poor prognosis influenced the selection of high- or low-dose regimens.
Keywords: bone metastases; long bones; oligometastasis; patterns of practice; postoperative radiation therapy.
© The Author(s) 2021. Published by Oxford University Press on behalf of The Japanese Radiation Research Society and Japanese Society for Radiation Oncology.
Figures
References
-
- Schulman KL, Kohles J. Economic burden of metastatic bone disease in the U.S. Cancer 2007;109:2334–42. - PubMed
-
- Chow E, Nguyen J, Zhang L et al. International field-testing of the reliability and validity of the EORTC QLQ-BM22 module to assess health-related quality of life in patients with bone metastases. Cancer 2012;118:1457–65. - PubMed
-
- Tubiana-Hulin M. Incidence, prevalence and distribution of bone metastases. Bone 1991;12:S9–10. - PubMed
-
- Rich SE, Chow R, Raman S et al. Update of the systematic review of palliative radiation therapy fractionation for bone metastases. Radiother Oncol 2018;126:547–57. - PubMed
-
- Saito T, Toya R, Oya N. Pain response rates after conventional radiation therapy for bone metastases in prospective nonrandomized studies: A systematic review. Pract Radiat Oncol 2019;9:81–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
