

N-glycan signature of serum immunoglobulins as a diagnostic biomarker of urothelial carcinomas
- PMID: 33455069
- PMCID: PMC7926015
- DOI: 10.1002/cam4.3727
N-glycan signature of serum immunoglobulins as a diagnostic biomarker of urothelial carcinomas
Abstract
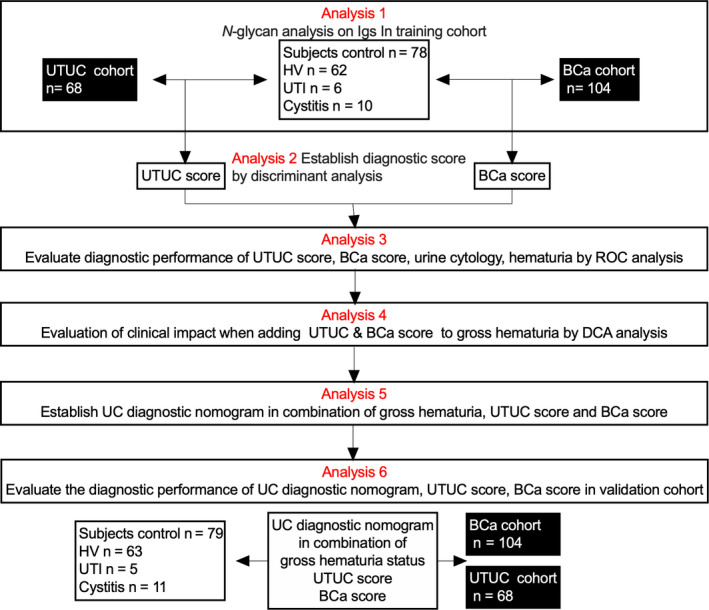
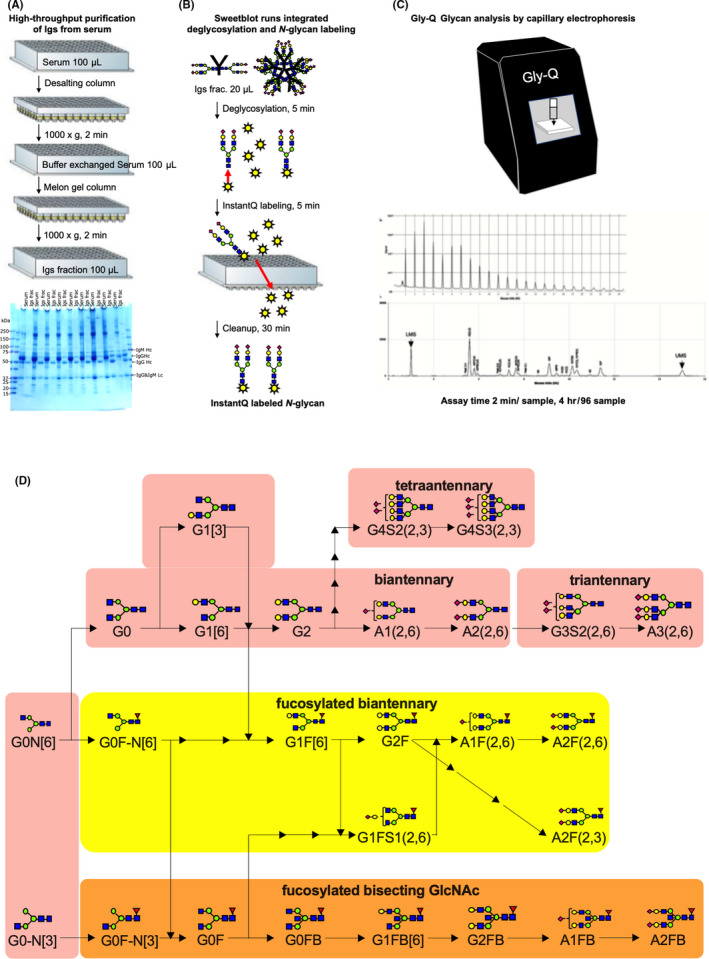
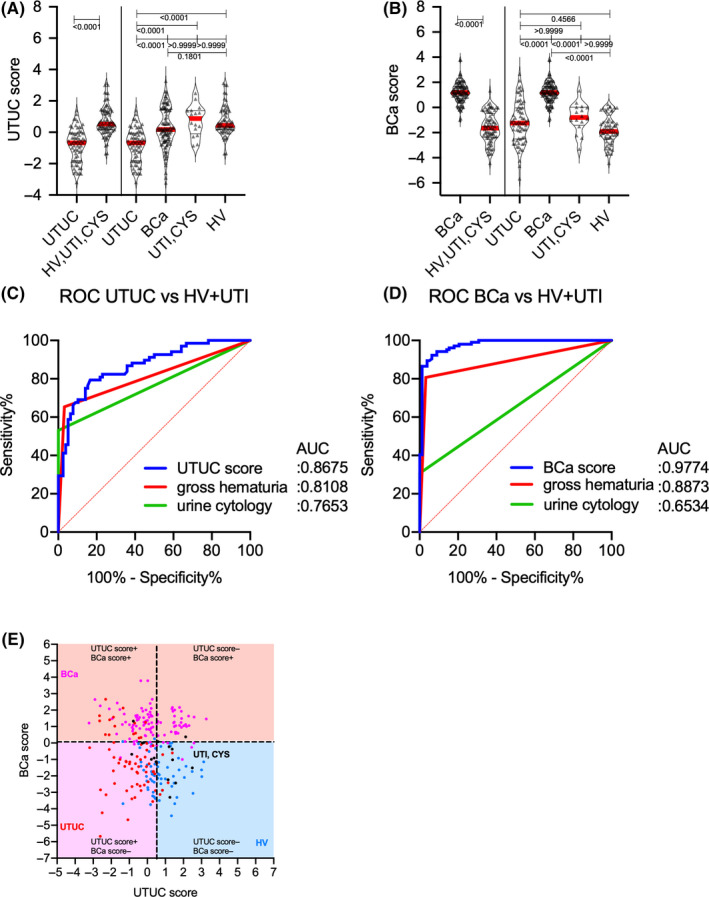
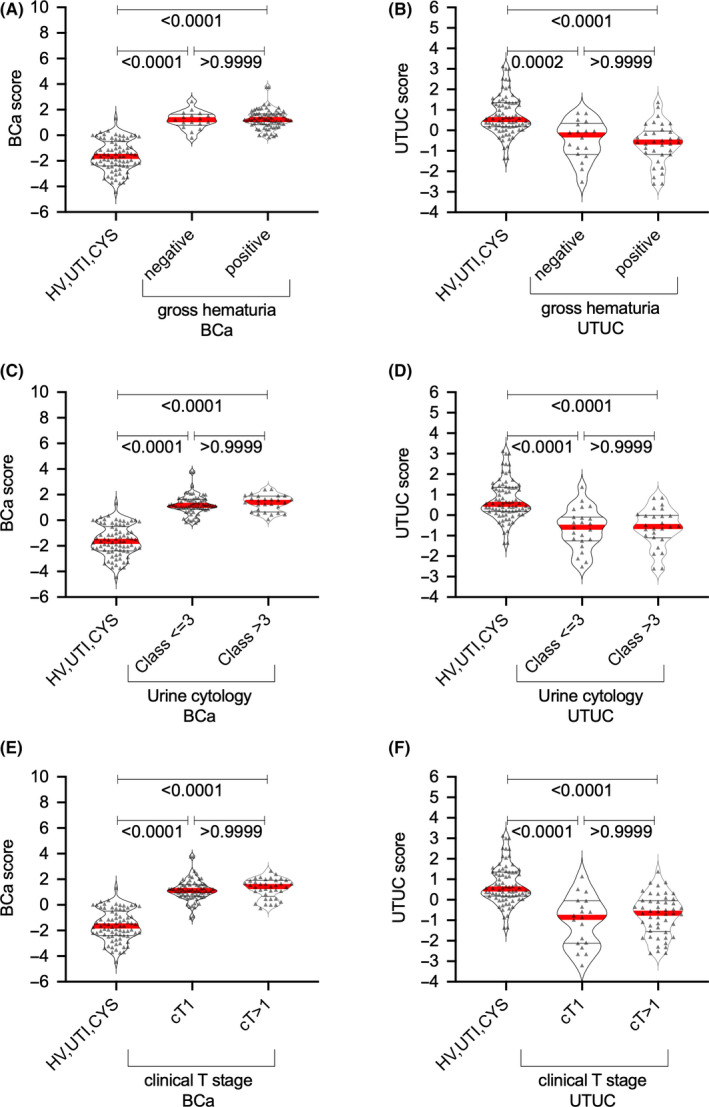
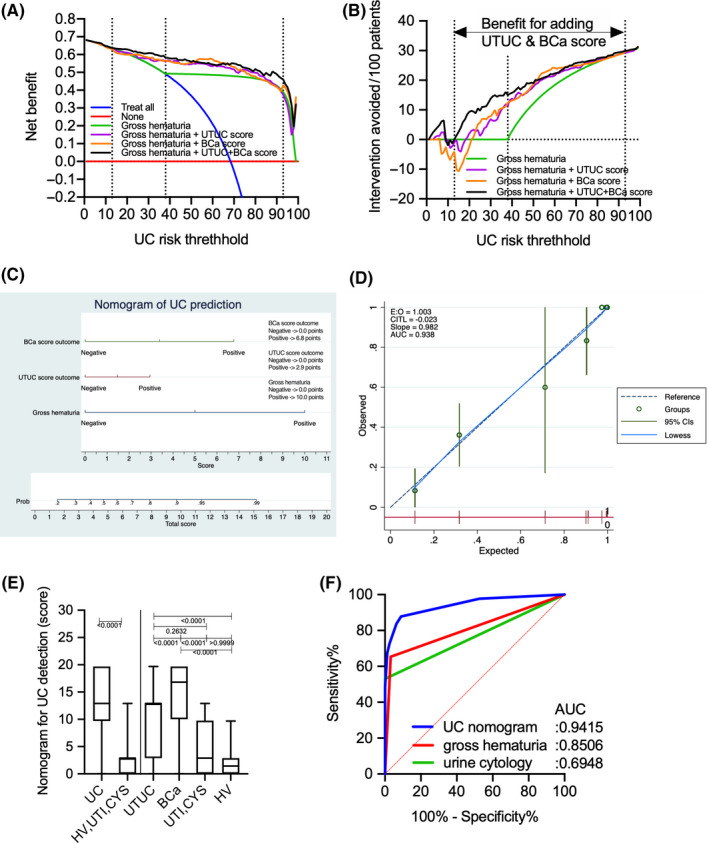
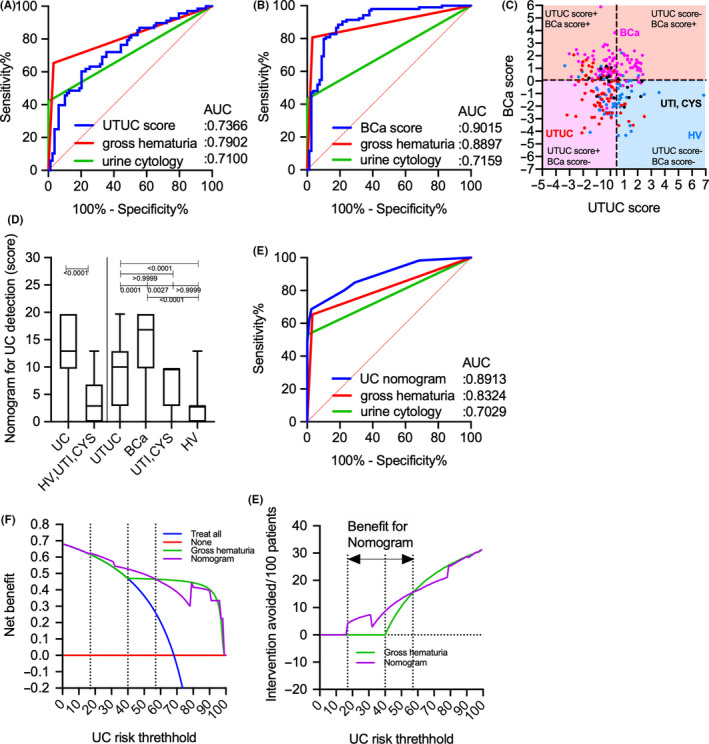
Discriminating between urothelial carcinoma (UC), including bladder cancer (BCa) and upper urinary tract UC (UTUC), is often challenging. Thus, the current study evaluated the diagnostic performance of N-glycosylation signatures of immunoglobulins (Igs) for detecting UC, including BCa and UTUC. N-glycosylation signatures of Igs from serum samples of the training cohort, including 104 BCa, 68 UTUC, 10 urinary tract infection, and 5 cystitis cases, as well as 62 healthy volunteers, were measured retrospectively using automated capillary-electrophoresis-based N-glycomics. UTUC or BCa scores were then established through discriminant analysis using N-glycan signatures of Igs. Diagnostic performance was evaluated using the area under receiver operating characteristics curve (AUC) and decision curve analyses (DCA). Our result showed that BCa and UTUC scores for discriminating BCa (AUC: 0.977) and UTUC (AUC: 0.867), respectively, provided significantly better clinical performance compared to urine cytology, gross hematuria, or clinical T1 cases. DCA revealed that adding BCa and UTUC scores to gross hematuria status was the best combination for detecting UC and avoiding the need for more intervention without overlooking UC (risk threshold: 13%-93%). The UC nomogram based on the combination of gross hematuria, UTUC score, and BCa score could detect UC with an AUC of 0.891, indicating significantly better performance compared to gross hematuria status in the validation cohort (251 patients). The limitations of this study include its small sample size and retrospective nature. The UC nomogram based on gross hematuria and N-glycosylation signatures of Igs can be a promising approach for the diagnosis of UC.
Keywords: N-glycosylation signatures; capillary-electrophoresis; diagnostic biomarker; immunogloburins; urothelial carcinoma.
© 2021 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors have no conflicts of interest.
Figures
References
-
- Park JC, Hahn NM. Bladder cancer: a disease ripe for major advances. Clin Adv Hematol Oncol. 2014;12:838‐845. - PubMed
-
- Munoz JJ, Ellison LM. Upper tract urothelial neoplasms: incidence and survival during the last 2 decades. J Urol. 2000;164:1523‐1525. - PubMed
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10‐29. - PubMed
-
- Inman BA, Tran VT, Fradet Y, Lacombe L. Carcinoma of the upper urinary tract: predictors of survival and competing causes of mortality. Cancer. 2009;115:2853‐2862. - PubMed
-
- Cowan NC. CT urography for hematuria. Nat Rev Urol. 2012;9:218‐226. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
