

TRPM2 in ischemic stroke: Structure, molecular mechanisms, and drug intervention
- PMID: 33455532
- PMCID: PMC7833771
- DOI: 10.1080/19336950.2020.1870088
TRPM2 in ischemic stroke: Structure, molecular mechanisms, and drug intervention
Abstract
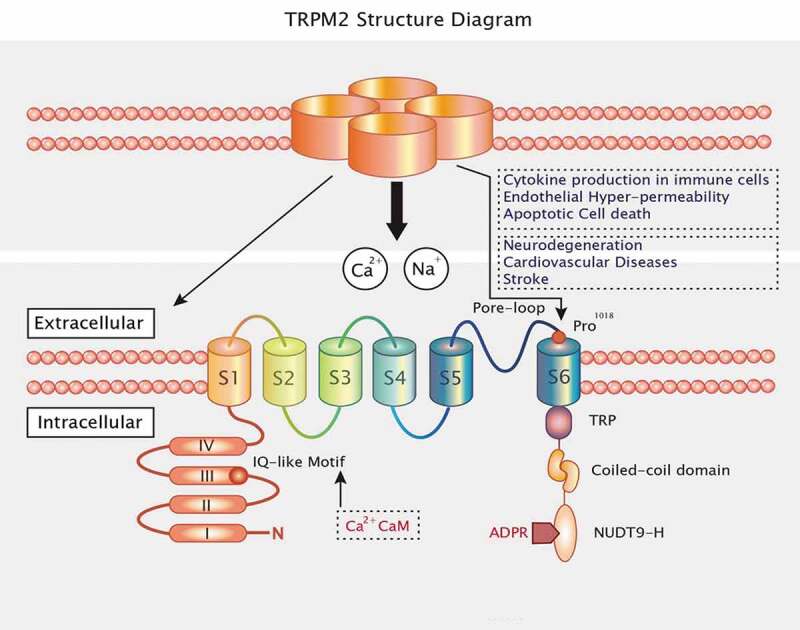
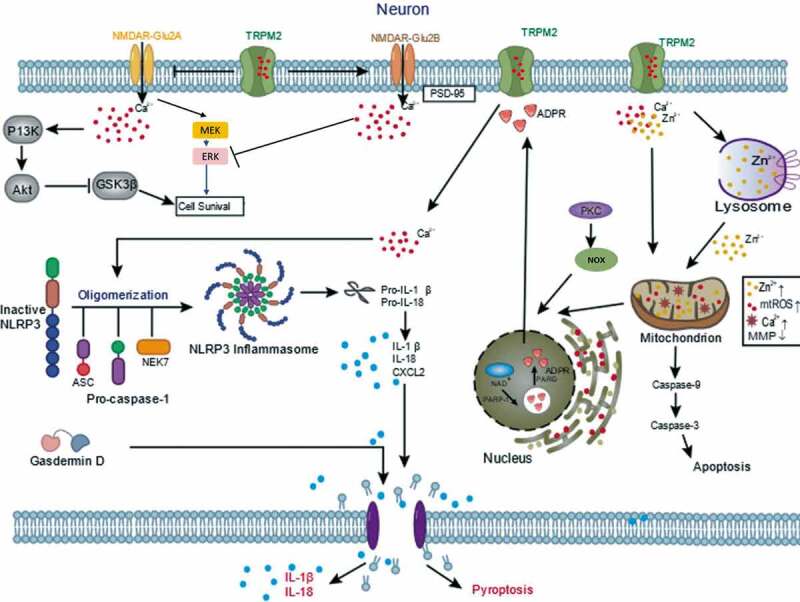
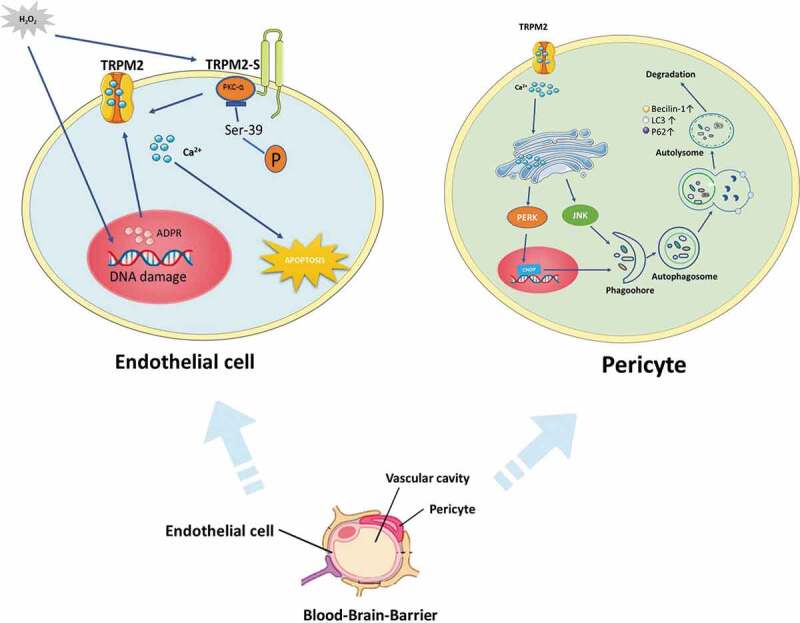
Ischemic stroke has a high lethality rate worldwide, and novel treatments are limited. Calcium overload is considered to be one of the mechanisms of cerebral ischemia. Transient receptor potential melastatin 2 (TRPM2) is a reactive oxygen species (ROS)-sensitive calcium channel. Cerebral ischemia-induced TRPM2 activation triggers abnormal intracellular Ca2+ accumulation and cell death, which in turn causes irreversible brain damage. Thus, TRPM2 has emerged as a new therapeutic target for ischemic stroke. This review provides data on the expression, structure, and function of TRPM2 and illustrates its cellular and molecular mechanisms in ischemic stroke. Natural and synthetic TRPM2 inhibitors (both specific and nonspecific) are also summarized. The three-dimensional protein structure of TRPM2 has been identified, and we speculate that molecular simulation techniques will be essential for developing new drugs that block TRPM2 channels. These insights about TRPM2 may be the key to find potent therapeutic approaches for the treatment of ischemic stroke.
Keywords: TRPM2 blockers; TRPM2 channel; ischemic stroke; pathogenesis; virtual screening.
Conflict of interest statement
No potential conflict of interest was reported by the authors.
Figures


References
-
- Beal CC. Gender and stroke symptoms: a review of the current literature. J Neurosci Nurs. 2010. April;42(2):80–87. - PubMed
-
- Strong K, Mathers C, Bonita R. Preventing stroke: saving lives around the world. Lancet Neurol. 2007;6(2):182–187. - PubMed
-
- Schwamm L, Ali S, Reeves M, et al. Temporal trends in patient characteristics and treatment with intravenous thrombolysis among acute ischemic stroke patients at get with the guidelines-stroke hospitals. Circ Cardiovasc Qual Outcomes. 2013;6(5):543–549. - PubMed
-
- Khoshnam S, Winlow W, Farzaneh M, et al. Pathogenic mechanisms following ischemic stroke. Neurol Sci. 2017;38(7):1167–1186. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous