

Compressed sensing time-of-flight magnetic resonance angiography with high spatial resolution for evaluating intracranial aneurysms: comparison with digital subtraction angiography
- PMID: 33455533
- PMCID: PMC8165900
- DOI: 10.1177/1971400920988099
Compressed sensing time-of-flight magnetic resonance angiography with high spatial resolution for evaluating intracranial aneurysms: comparison with digital subtraction angiography
Abstract
Background and purpose: Compressed sensing is used for accelerated acquisitions with incoherently under-sampled k-space data, and intracranial time-of-flight magnetic resonance angiography is suitable for compressed sensing. Compressed sensing time-of-flight is beneficial in decreasing acquisition time and increasing spatial resolution while maintaining acquisition time. In this retrospective study, we aimed to evaluate the image quality and diagnostic performance of compressed sensing time-of-flight with high spatial resolution and compare with parallel imaging time-of-flight using digital subtraction angiography as a reference.
Material and methods: In total, 39 patients with 46 intracranial aneurysms underwent parallel imaging and compressed sensing time-of-flight in the same imaging session and digital subtraction angiography before or after magnetic resonance angiography. The overall image quality, artefacts and diagnostic confidence were assessed by two observers. The contrast ratio, maximal aneurysm diameters and diagnostic performance were evaluated.
Results: Compressed sensing time-of-flight showed significantly better overall image quality, degree of artefacts and diagnostic confidence in both observers, with better inter-observer agreement. The contrast ratio was significantly higher for compressed sensing time-of-flight than for parallel imaging time-of-flight in both observers (source images, P < 0.001; maximum intensity projection images, P < 0.05 for both observers); however, the measured maximal diameters of aneurysms were not significantly different. Compressed sensing time-of-flight showed higher sensitivity, specificity, accuracy and positive and negative predictive values for detecting aneurysms than parallel imaging time-of-flight in both observers, with better inter-observer agreement. Compressed sensing time-of-flight was preferred over parallel imaging time-of-flight by both observers; however, parallel imaging time-of-flight was preferred in cases of giant and large aneurysms.
Conclusions: Compressed sensing-time-of-flight provides better image quality and diagnostic performance than parallel imaging time-of-flight. However, neuroradiologists should be aware of under-sampling artefacts caused by compressed sensing.
Keywords: Compressed sensing; cerebral aneurysm; time-of-flight magnetic resonance angiography.
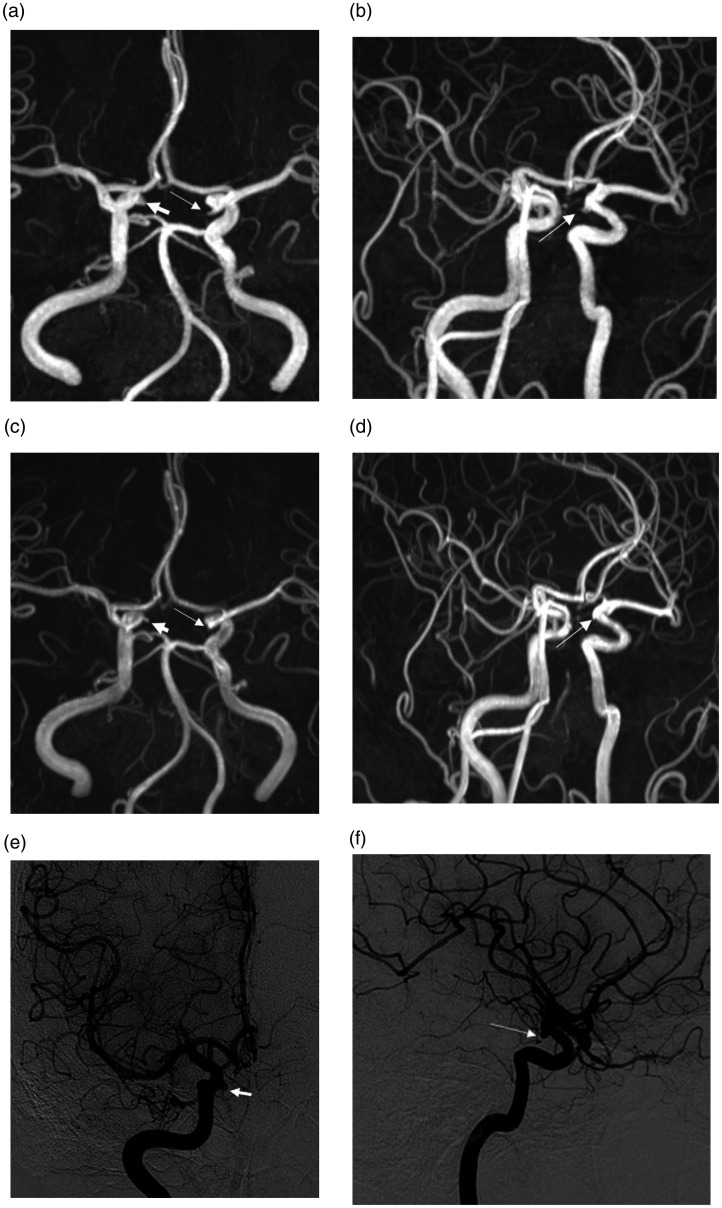
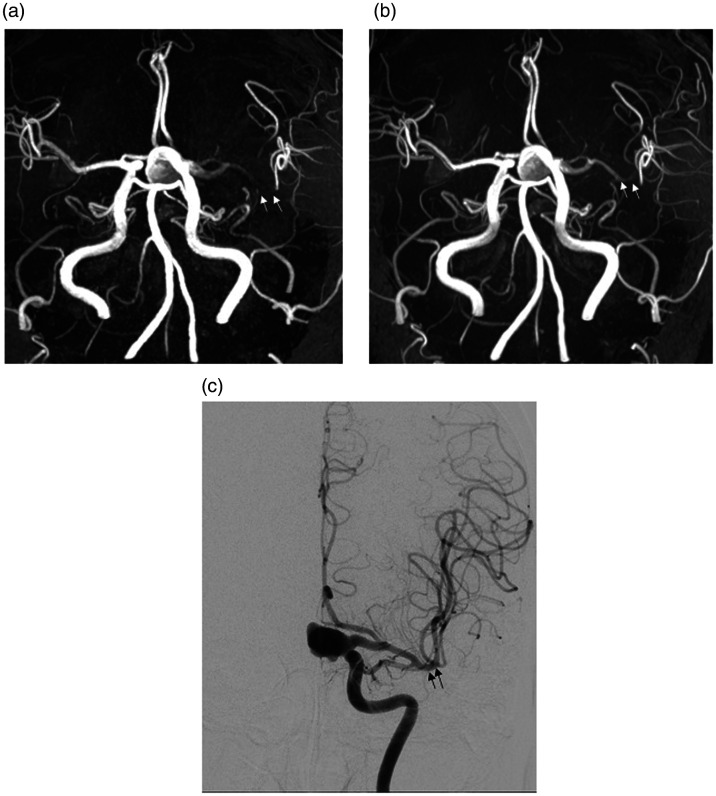
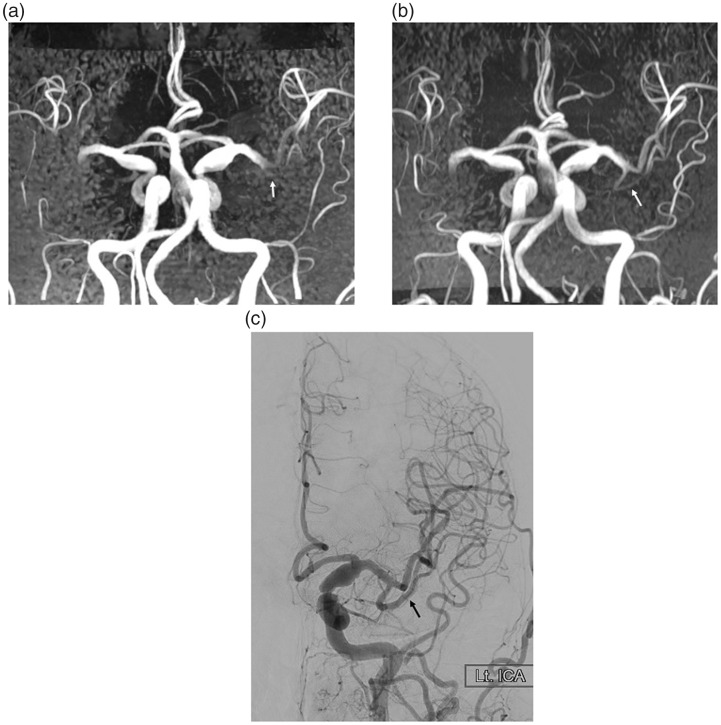
Figures
Similar articles
-
Added diagnostic values of three-dimensional high-resolution proton density-weighted magnetic resonance imaging for unruptured intracranial aneurysms in the circle-of-Willis: Comparison with time-of-flight magnetic resonance angiography.PLoS One. 2020 Dec 3;15(12):e0243235. doi: 10.1371/journal.pone.0243235. eCollection 2020. PLoS One. 2020. PMID: 33270756 Free PMC article.
-
Follow-Up Assessment of Intracranial Aneurysms Treated with Endovascular Coiling: Comparison of Compressed Sensing and Parallel Imaging Time-of-Flight Magnetic Resonance Angiography.Tomography. 2022 Jun 18;8(3):1608-1617. doi: 10.3390/tomography8030133. Tomography. 2022. PMID: 35736881 Free PMC article.
-
A comparison between magnetic resonance angiography at 3 Teslas (time-of-flight and contrast-enhanced) and flat-panel digital subtraction angiography in the assessment of embolized brain aneurysms.Clinics (Sao Paulo). 2011;66(4):641-8. doi: 10.1590/s1807-59322011000400020. Clinics (Sao Paulo). 2011. PMID: 21655760 Free PMC article.
-
Comprehensive review of imaging of intracranial aneurysms and angiographically negative subarachnoid hemorrhage.Neurosurg Focus. 2019 Dec 1;47(6):E20. doi: 10.3171/2019.9.FOCUS19653. Neurosurg Focus. 2019. PMID: 31786554 Review.
-
Intracranial aneurysm detection: an object detection perspective.Int J Comput Assist Radiol Surg. 2024 Sep;19(9):1667-1675. doi: 10.1007/s11548-024-03132-z. Epub 2024 Apr 17. Int J Comput Assist Radiol Surg. 2024. PMID: 38632166 Review.
Cited by
-
Observation of intracranial artery and venous sinus hemodynamics using compressed sensing-accelerated 4D flow MRI: performance at different acceleration factors.Front Neurosci. 2024 Jul 25;18:1438003. doi: 10.3389/fnins.2024.1438003. eCollection 2024. Front Neurosci. 2024. PMID: 39119457 Free PMC article.
-
Ultra-High-Resolution Time-of-Flight MR-Angiography for the Noninvasive Assessment of Intracranial Aneurysms, Alternative to Preinterventional DSA?Clin Neuroradiol. 2023 Dec;33(4):1115-1122. doi: 10.1007/s00062-023-01320-z. Epub 2023 Jul 4. Clin Neuroradiol. 2023. PMID: 37401949 Free PMC article.
-
Intelligent Algorithm-Based Multislice Spiral Computed Tomography to Diagnose Coronary Heart Disease.Comput Math Methods Med. 2022 Jan 13;2022:4900803. doi: 10.1155/2022/4900803. eCollection 2022. Comput Math Methods Med. 2022. Retraction in: Comput Math Methods Med. 2023 Dec 6;2023:9896705. doi: 10.1155/2023/9896705. PMID: 35069783 Free PMC article. Retracted.
References
-
- Oelerich M, Lentschig M, Zunker P, et al.. Intracranial vascular stenosis and occlusion: comparison of 3D time-of-flight and 3D phase-contrast MR angiography. Neuroradiology 1998; 40: 567–573. - PubMed
-
- Mönninghoff C, Maderwald S, Theysohn J, et al.. Evaluation of intracranial aneurysms with 7 T versus 1.5 T time-of-flight MR angiography – initial experience. Rofo 2009; 181(1): 16–23. - PubMed
-
- Li M-H, Li Y-D, Tan H-Q, et al.. Contrast-free MRA at 3.0 T for the detection of intracranial aneurysms. Neurology 2011; 77: 667–676. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
