

Percutaneous mechanical thrombectomy in acute and subacute lower-extremity ischemia: impact of adjunctive, solely nonthrombolytic endovascular procedures
- PMID: 33455896
- PMCID: PMC7963386
- DOI: 10.5152/dir.2021.19403
Percutaneous mechanical thrombectomy in acute and subacute lower-extremity ischemia: impact of adjunctive, solely nonthrombolytic endovascular procedures
Abstract
Purpose: We aimed to evaluate the role of adjunctive, solely nonthrombolytic endovascular therapy in treatment of acute lower-extremity ischemia by rotational percutaneous mechanical thrombectomy.
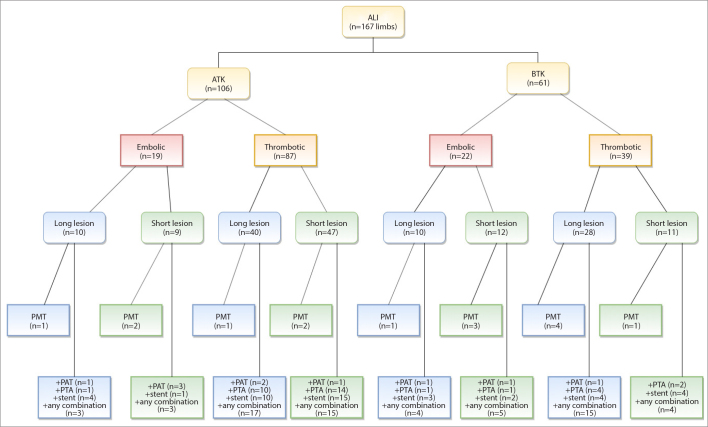
Methods: A retrospective, single-center evaluation of 165 patients (167 limbs) that underwent rotational percutaneous mechanical thrombectomy between 2009 and 2016 was performed.
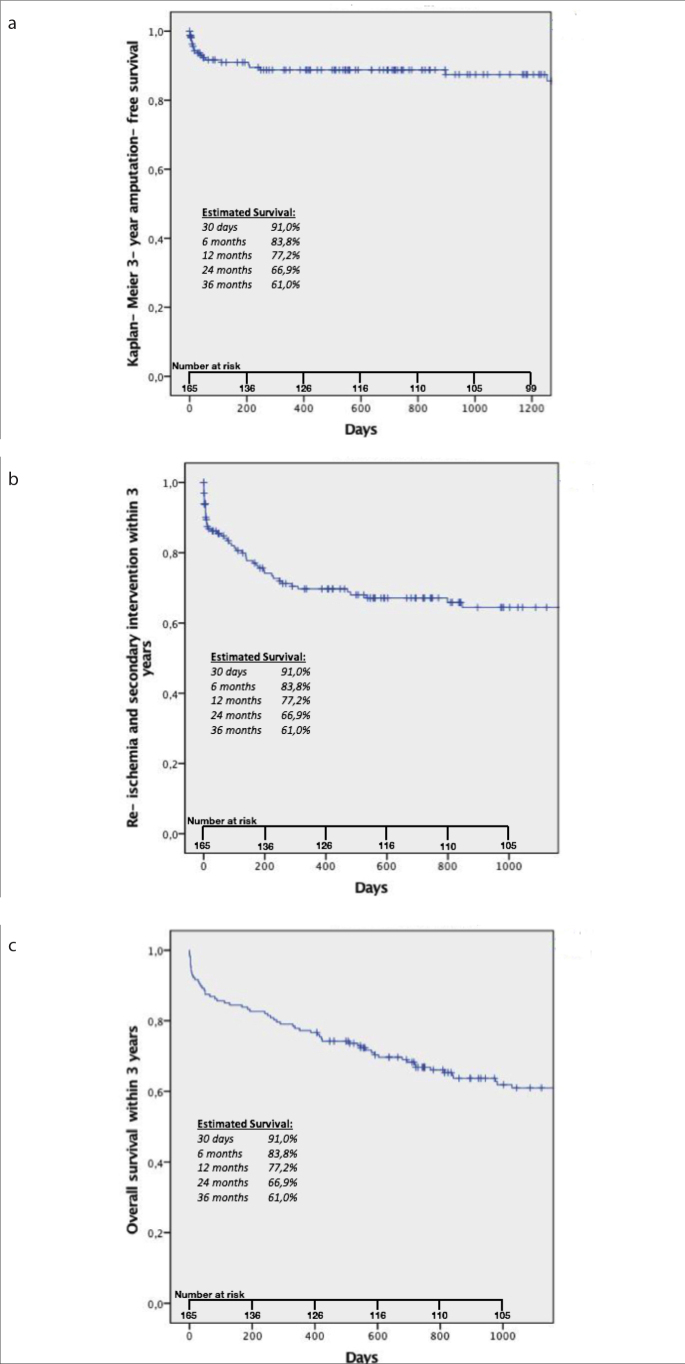
Results: Rotational percutaneous mechanical thrombectomy was used as a single therapy in 9.0% (15 limbs), followed by percutaneous aspiration thrombectomy in 6.0% (10 limbs), percutaneous transluminal angioplasty in 19.8% (33 limbs) and stenting in 25.7% (43 limbs). Rotational percutaneous mechanical thrombectomy was followed by any combination of these three interventions in 39.5%. Clinical and technical success was documented in 92.2%, complications in 10.3% (n=17). No significant difference in clinical and technical success was observed using rotational percutaneous mechanical thrombectomy alone or with additional endovascular therapy. On a long-term basis, the re-ischemia-free survival was nearly twice as high as in previous studies that reported more cases treated by rotational percutaneous mechanical thrombectomy alone.
Conclusion: To assure a long-lasting primary patency after percutaneous mechanical thrombectomy, concomitant treatment of underlying lesions with adjunctive, nonthrombolytic endovascular methods should be considered.
Conflict of interest statement
The authors declared no conflicts of interest.
Figures

Similar articles
-
Single-session aspiration thrombectomy of lower extremity deep vein thrombosis using large-size catheter without pharmacologic thrombolysis.Cardiovasc Intervent Radiol. 2014 Apr;37(2):412-9. doi: 10.1007/s00270-013-0676-1. Epub 2013 Jun 21. Cardiovasc Intervent Radiol. 2014. PMID: 23793745
-
Aggressive percutaneous mechanical thrombectomy of deep venous thrombosis: early clinical results.Arch Surg. 2007 Jun;142(6):513-8; discussion 518-9. doi: 10.1001/archsurg.142.6.513. Arch Surg. 2007. PMID: 17576886
-
Percutaneous Mechanical Thromboembolectomy in Acute Lower Limb Ischemia.Cardiovasc Intervent Radiol. 2019 Feb;42(2):178-185. doi: 10.1007/s00270-018-2129-3. Epub 2018 Nov 28. Cardiovasc Intervent Radiol. 2019. PMID: 30488304
-
Endovascular treatment of acute limb ischemia and proximal deep vein thrombosis using rotational thrombectomy: A review of published literature.Cardiovasc Revasc Med. 2013 Nov-Dec;14(6):343-8. doi: 10.1016/j.carrev.2013.08.005. Epub 2013 Sep 21. Cardiovasc Revasc Med. 2013. PMID: 24060441 Review.
-
Percutaneous Rotational Mechanical Atherectomy Plus Thrombectomy Using Rotarex S Device in Patients With Acute and Subacute Lower Limb Ischemia: A Review of Safety, Efficacy, and Outcomes.Front Cardiovasc Med. 2020 Oct 22;7:557420. doi: 10.3389/fcvm.2020.557420. eCollection 2020. Front Cardiovasc Med. 2020. PMID: 33195452 Free PMC article. Review.
Cited by
-
Percutaneous Thrombectomy for the Treatment of Lower Extremity Deep Vein Thrombosis: Medium-Term Follow-up Results and Analysis of 112 Cases.Cureus. 2022 Feb 28;14(2):e22689. doi: 10.7759/cureus.22689. eCollection 2022 Feb. Cureus. 2022. PMID: 35371750 Free PMC article.
-
Percutaneous Thrombectomy in Patients with Occlusions of the Aortoiliac Segment: A Case Series.Cardiovasc Intervent Radiol. 2022 Nov;45(11):1684-1692. doi: 10.1007/s00270-022-03222-y. Epub 2022 Aug 24. Cardiovasc Intervent Radiol. 2022. PMID: 36002537 Free PMC article.
References
-
- Working Party on Thrombolysis in the Management of Limb Ischemia b Thrombolysis in the management of lower limb peripheral arterial occlusion-a consensus document. Working Party of Thrombolysis in the Management of Limb Ischemia. Am J Cardiol. 1998;81:207–218. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
