

Development and temporal external validation of a simple risk score tool for prediction of outcomes after severe head injury based on admission characteristics from level-1 trauma centre of India using retrospectively collected data
- PMID: 33455929
- PMCID: PMC7813344
- DOI: 10.1136/bmjopen-2020-040778
Development and temporal external validation of a simple risk score tool for prediction of outcomes after severe head injury based on admission characteristics from level-1 trauma centre of India using retrospectively collected data
Abstract
Objective: To develop and validate a simple risk scores chart to estimate the probability of poor outcomes in patients with severe head injury (HI).
Design: Retrospective.
Setting: Level-1, government-funded trauma centre, India.
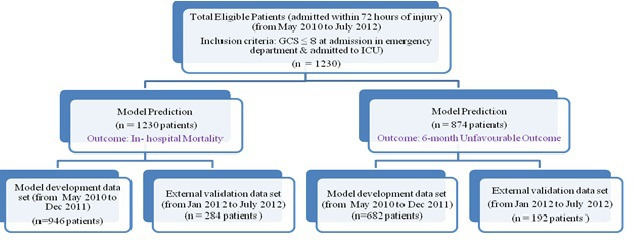
Participants: Patients with severe HI admitted to the neurosurgery intensive care unit during 19 May 2010-31 December 2011 (n=946) for the model development and further, data from same centre with same inclusion criteria from 1 January 2012 to 31 July 2012 (n=284) for the external validation of the model.
Outcomes: In-hospital mortality and unfavourable outcome at 6 months.
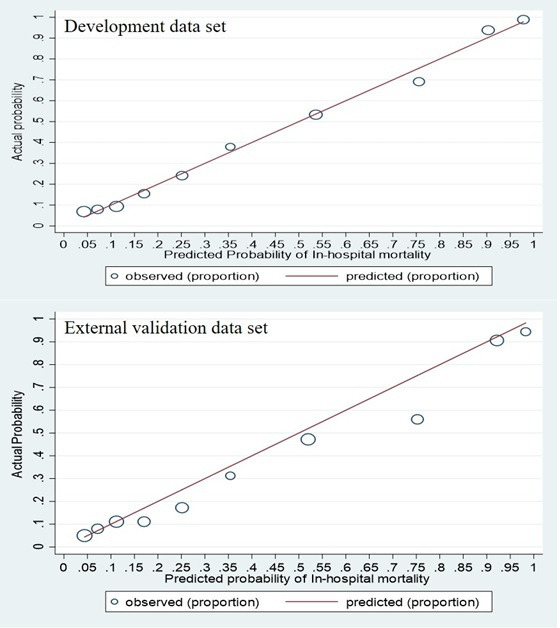
Results: A total of 39.5% and 70.7% had in-hospital mortality and unfavourable outcome, respectively, in the development data set. The multivariable logistic regression analysis of routinely collected admission characteristics revealed that for in-hospital mortality, age (51-60, >60 years), motor score (1, 2, 4), pupillary reactivity (none), presence of hypotension, basal cistern effaced, traumatic subarachnoid haemorrhage/intraventricular haematoma and for unfavourable outcome, age (41-50, 51-60, >60 years), motor score (1-4), pupillary reactivity (none, one), unequal limb movement, presence of hypotension were the independent predictors as its 95% confidence interval (CI) of odds ratio (OR)_did not contain one. The discriminative ability (area under the receiver operating characteristic curve (95% CI)) of the score chart for in-hospital mortality and 6 months outcome was excellent in the development data set (0.890 (0.867 to 912) and 0.894 (0.869 to 0.918), respectively), internal validation data set using bootstrap resampling method (0.889 (0.867 to 909) and 0.893 (0.867 to 0.915), respectively) and external validation data set (0.871 (0.825 to 916) and 0.887 (0.842 to 0.932), respectively). Calibration showed good agreement between observed outcome rates and predicted risks in development and external validation data set (p>0.05).
Conclusion: For clinical decision making, we can use of these score charts in predicting outcomes in new patients with severe HI in India and similar settings.
Keywords: public health; statistics & research methods; trauma management.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures





References
-
- WHO . World health report 2003-shaping the future. Geneva: Worald Health Organization, 2003.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical