

A service evaluation of transport destination and outcome of patients with post-ROSC STEMI in an English ambulance service
- PMID: 33456384
- PMCID: PMC7783911
- DOI: 10.29045/14784726.2020.06.5.1.32
A service evaluation of transport destination and outcome of patients with post-ROSC STEMI in an English ambulance service
Abstract
Background: In the UK, there are approximately 60,000 cases of out-of-hospital cardiac arrest (OHCA) each year. There is mounting evidence that post-resuscitation care should include early angiography and primary percutaneous coronary intervention (pPCI) in cases of OHCA where a cardiac cause is suspected. Yorkshire Ambulance Service (YAS) staff can transport patients with a return of spontaneous circulation (ROSC) directly to a pPCI unit if their post-ROSC ECG shows evidence of ST elevation myocardial infarction (STEMI). This service evaluation aimed to determine the factors that affect the transport destination, hospital characteristics and 30-day survival rates of post-ROSC patients with presumed cardiac aetiology.
Methods: All patient care records (PCRs) previously identified for the AIRWAYS-2 trial between January and July 2017 were reviewed. Patients were eligible for inclusion if they were an adult non-traumatic OHCA, achieved ROSC on scene and were treated and transported by (YAS). Descriptive statistics were used to analyse the data.
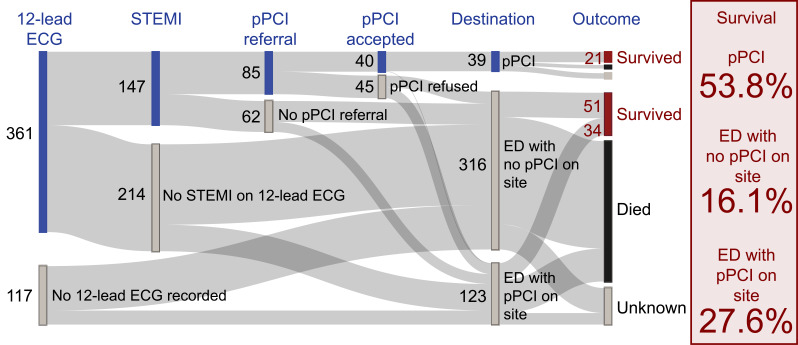
Results: 478 patients met the inclusion criteria. 361/478 (75.6%) patients had a post-ROSC ECG recorded, with 149/361 (41.3%) documented cases of STEMI and 88/149 (59.1%) referred to a pPCI unit by the attending clinicians. 40/88 (45.5%) of referrals made were accepted by the pPCI units. Patients taken directly to pPCI were most likely to survive to 30 days (25/39, 53.8%), compared to patients taken to an emergency department (ED) at a pPCI-capable hospital (34/126, 27.0%), or an ED at a non-pPCI-capable hospital (50/310, 16.1%).
Conclusion: Staff should be encouraged to record a 12-lead ECG on all post-ROSC patients, and make a referral to the regional pPCI-capable centre if there is evidence of a STEMI, or a cardiac cause is likely, since 30-day survival is highest for patients who are taken directly for pPCI. Ambulance services should continue to work with regional pPCI-capable centres to ensure that suitable patients are accepted to maximise potential for survival.
Keywords: out-of-hospital cardiac arrest; pPCI; post-ROSC care.
© 2020 The Author(s).
Conflict of interest statement
None declared.
Figures
References
-
- Arabi A., Patel A., Al Suwaldi J., Gehani A., Singh R. & Albinali H. (2018). Clinical profile, management, and outcome in patients with out of hospital cardiac arrest (OHCA) and ST segment elevation myocardial infarction: Insights from a 20-year registry. Angiology, 69(3): 249–255. https://doi.org/10.1177/0003319717699500. - PubMed
-
- Choudry F. A., Weerackody R. P., Timmins A. D., Wragg A., Mathur A., Sporton S. & Jain A. K. (2015). Importance of primary percutaneous intervention for reducing mortality in ST-elevation myocardial infarction complicated by out of hospital cardiac arrest. European Heart Journal: Acute Cardiovascular Care, 4(4), 378–385. https://doi.org/10.1177/2048872614555990. - PubMed
-
- Deakin C. D., Fothergill R., Moore F., Watson L. & Whitbread M. (2014). Level of consciousness on admission to a heart attack centre is a predictor of survival from out-of-hospital cardiac arrest. Resuscitation, 85(7), 905–909. https://doi.org/10.1016/j.resuscitation.2014.02.020. - PubMed
-
- Dicker B., Todd V. F., Tunnage B., Swain A., Smith T. & Howie G. (2019). Direct transport to PCI-capable hospitals after out-of-hospital cardiac arrest in New Zealand: Inequities and outcomes. Resuscitation, 142, 111–116. https://doi.org/10.1016/j-resuscitation.2019.06.283. - PubMed
-
- Fisher M. B., Messerli A. & Whayne T. (2018). Characteristics, management, and results of Out-of-Hospital Cardiac Arrest (OHCA) with or without ST-Segment Elevation Myocardial Infarction (STEMI). Angiology, 69(3), 189–191. https://doi-org.libaccess.hud.ac.uk/10.1177/0003319717709686. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous