

Significant Clinical Associations Between Exposure Type Factors and Recurrent Wheezing and Asthma in Children
- PMID: 33456612
- PMCID: PMC7803326
- DOI: 10.25122/jml-2020-0143
Significant Clinical Associations Between Exposure Type Factors and Recurrent Wheezing and Asthma in Children
Abstract
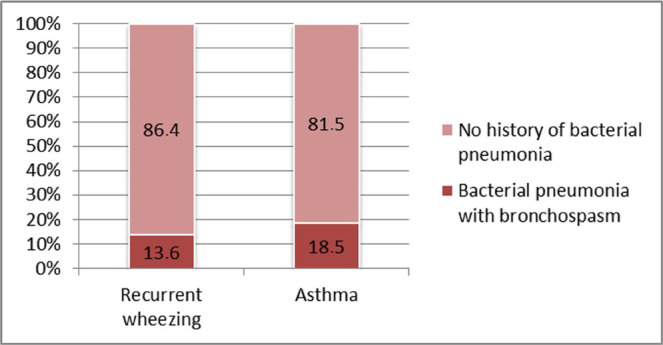
The study aimed to identify certain factors related to family history, pathological conditions, or exposure-type that are significantly correlated with recurrent wheezing and/or asthma in children. One hundred nine children with recurrent wheezing and 44 children with asthma were studied in order to identify the degree of correlation of these conditions with familial history of asthma or atopy, child's age group, gender, premature birth, perinatal asphyxia, neonatal infection, and antibiotic treatment during the neonatal period, history of atopy and obesity and histamine intolerance, nasopharyngeal bacterial colonization, pneumonia with bronchospasm. The clinical picture of these two diseases was also compared regarding the severity of exacerbations and their response to controller therapy. The medium age of children diagnosed with recurrent wheezing was significantly lower than those diagnosed with asthma (5.64 vs. 9.01 years; p<0.001). Inside the recurrent wheezing group, age distribution differed significantly from the asthma group (p-value <0.001). Atopy was the only pathological condition significantly associated with asthma (56.0%) when compared with the recurrent wheezing group (30.2%) with a relative risk value of 1.34 (p<0.004). For patients colonized with Staphylococcus aureus, the medium number of wheezing exacerbations was significantly higher (p<0.049). Approximately 91% of patients in the recurrent wheezing group and 71% from the asthma group responded to appropriate controller treatment. Our study showed a significant association between asthma and atopy, justifying the need to monitor asthma risk in a child with wheezing and atopy. Nasal carriage of Staphylococcus aureus proved to be significantly associated with the recurrence of wheezing in children.
Keywords: Recurrent wheezing; asthma; atopy; nasopharyngeal colonisation.
©Carol Davila University Press.
Figures
















References
-
- Gern JE, Jackson DJ, Lemanske jr RF, Seroogy CM, Tachinardi U, Craven M, Hwang SY, Hamilton CM, Huggins W, O’Connor GT, Gold DR, Miller R, Kattan M, Johnson C C, Ownby D, Zoratti EM, Wood RA, Visness CM, Martinez FM, Wright A, Lynch S, Ober C, Khurana Hershey GK, Ryan P, Hartert T. Bacharier LB: The Children’s Respiratory and Environmental Workgroup (CREW) birth cohort consortium: design, methods, and study population. Respiratory Research. 2019:20–115. doi: 10.1186/s12931-019-1088-9. - DOI - PMC - PubMed
-
- Taussig LM, Wright AL, Holberg CJ, Halonen M, Morgan WJ, Martinez F. Tucson Children’s Respiratory Study: 1980 to present. J Allergy Clin Immunol. 2003;111(4):661–675. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical