

Review
doi: 10.1016/j.bjae.2018.06.005.
Epub 2018 Aug 31.
Brain imaging for anaesthetists and intensivists: part 1-computed tomography
Affiliations
- PMID: 33456794
- PMCID: PMC7808021
- DOI: 10.1016/j.bjae.2018.06.005
Item in Clipboard
Review
Brain imaging for anaesthetists and intensivists: part 1-computed tomography
BJA Educ.
2018 Oct.
No abstract available
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
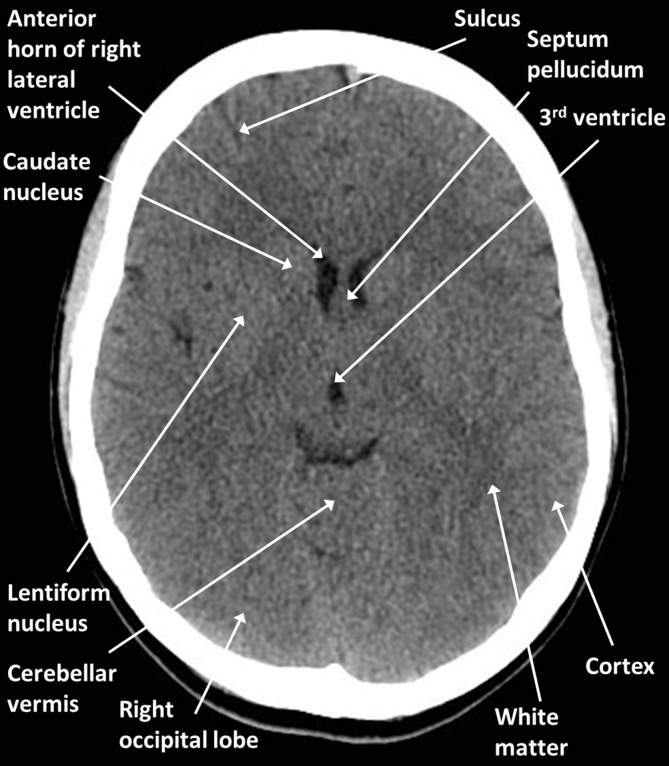
Brain anatomy: axial CT at the level of the third ventricle.
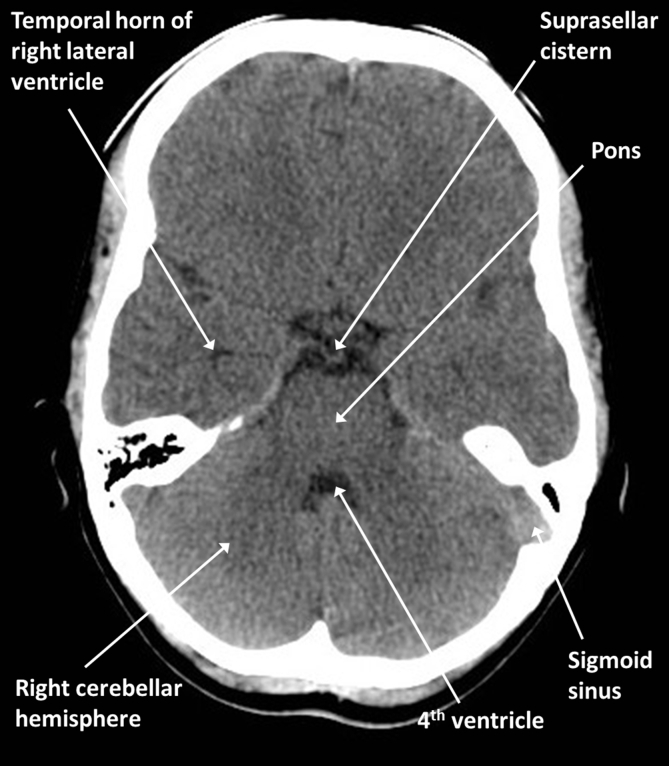
Brain anatomy: axial CT at the level of the basal cisterns.
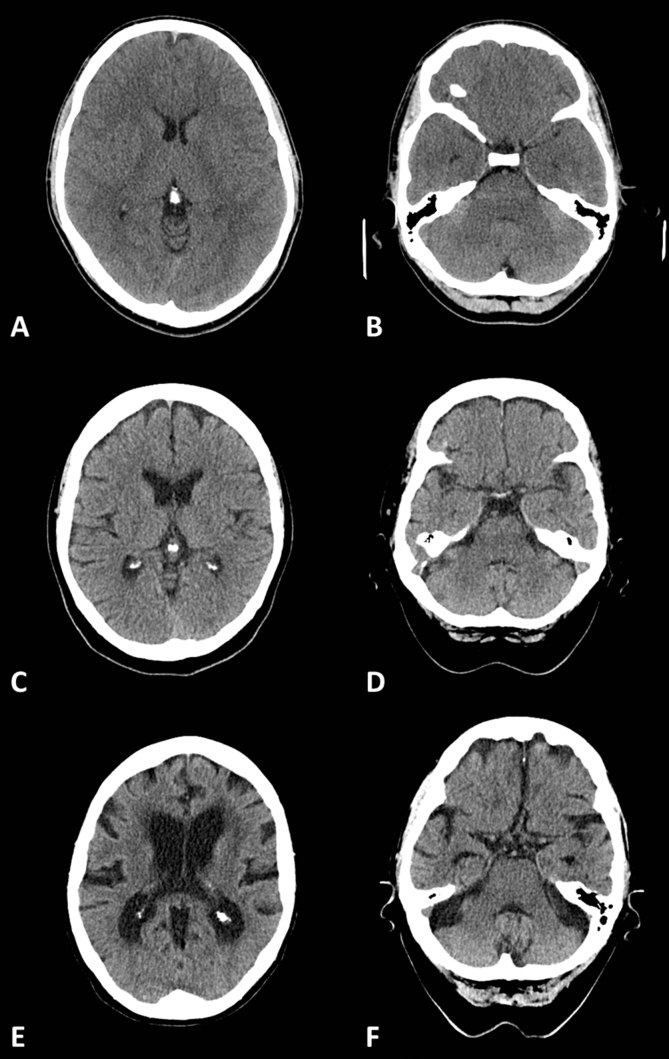
Brain atrophy with normal ageing: (A, B) 20 yr old; (C, D) 60 yr old; and (E, F) 90 yr old.
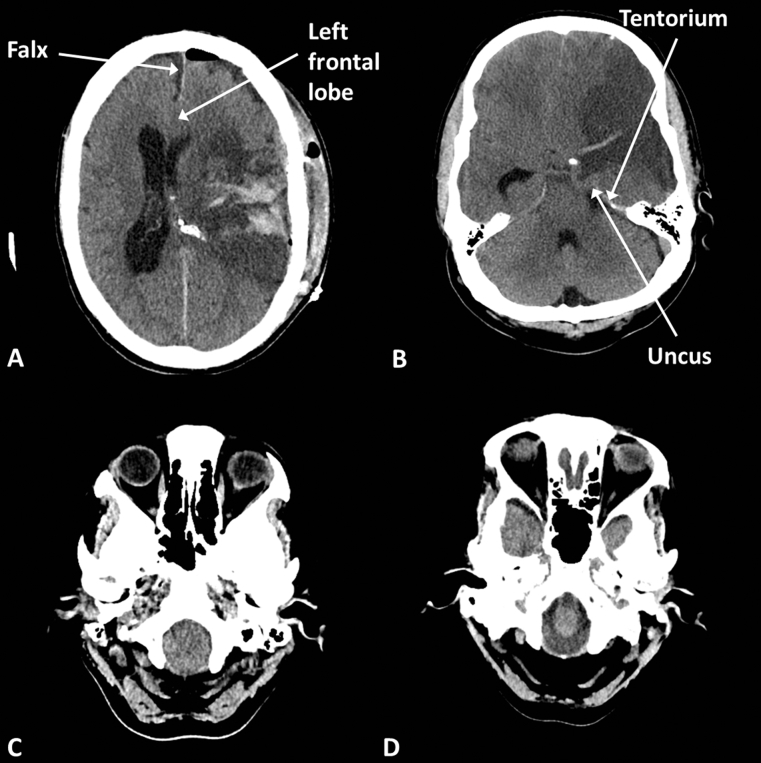
Brain herniations. (A) Postoperative haematoma causing subfalcine herniation, the left frontal lobe bulges beneath the falx; (B) left middle cerebral artery (MCA) infarct (notice the dense vessel and loss of grey/white differentiation) causing uncal herniation, the left uncus bulges over the tentorium; (C) tonsillar herniation, the cerebellar tonsils bulge into the foramen magnum; and (D) normal foramen magnum with CSF visible around the medulla.
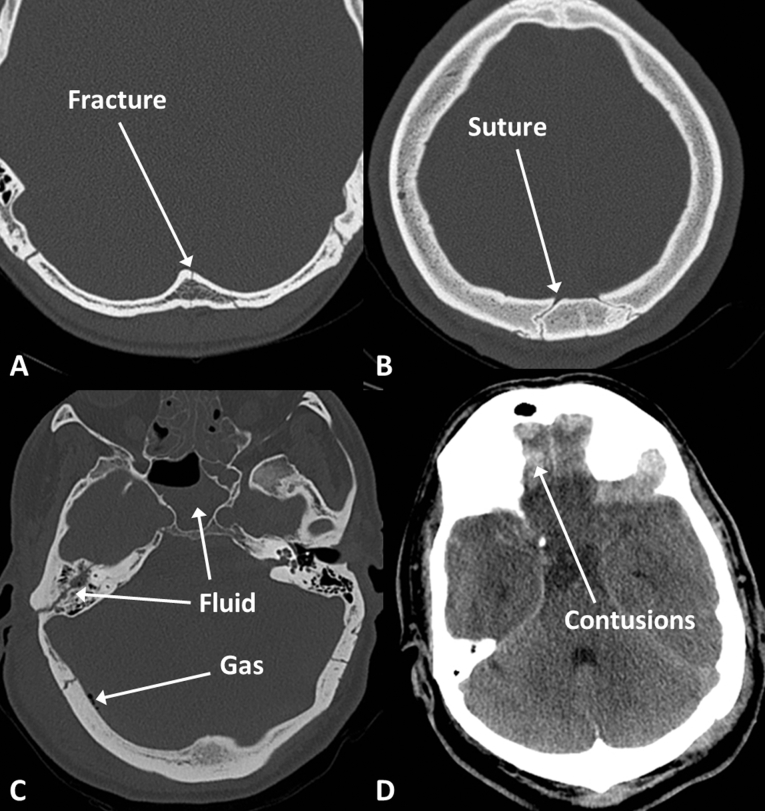
Fractures and contusions. (A) Linear fracture; (B) suture line; (C) fluid in the mastoid air cells and sphenoid sinus suggesting skull base fracture, pneumocephalus indicated by gas density within the cranium; and (D) frontal contusions indicated by high density within the brain parenchyma.
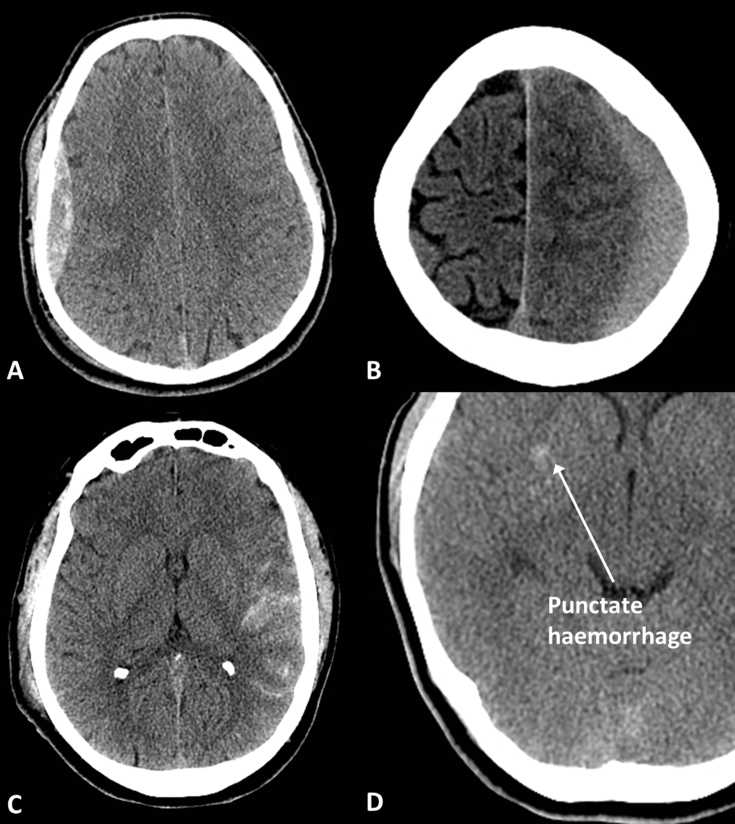
Traumatic haemorrhage. (A) Extradural haematoma; (B) subdural haematoma; (C) subarachnoid haemorrhage; and (D) subtle punctate haemorrhage indicating diffuse axonal injury.

Non-traumatic haemorrhage. (A) Hypertensive basal ganglia haemorrhage; (B) lobar haemorrhage in amyloid angiopathy; and (C) well-defined haemorrhagic metastasis in right frontal lobe; notice the low density (oedema) in the left frontal lobe which was related to another lesion on a lower slice.
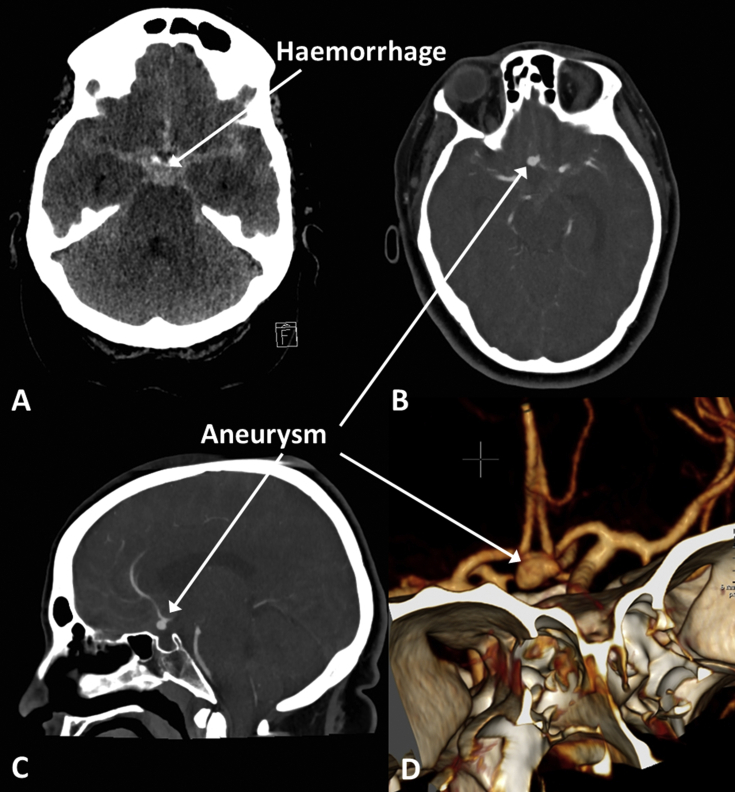
Aneurysmal subarachnoid haemorrhage. (A) High-density acute blood fills the basal cisterns; (B) axial CT angiogram (CTA) showing anterior communicating artery (Acom) aneurysm; (C) sagittal CTA showing Acom aneurysm; and (D) 3D surface rendered reconstruction of CTA showing Acom aneurysm.
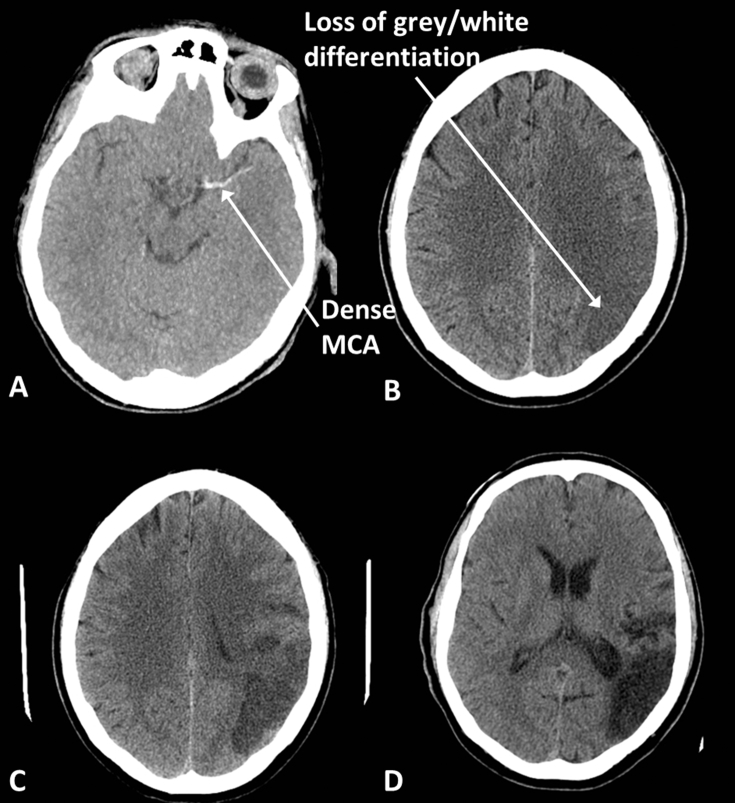
Middle cerebral artery (MCA) infarction. (A) Acute thrombus within the MCA appears dense. (B) Early infarcts, here 3 h after symptom onset in a different patient to (A), are seen as loss of grey/white differentiation and swelling; notice that fewer sulci are visible on the left compared with the right. (C) With time the infarcted tissue becomes less dense and more obvious, here at 36 h. (D) Chronic infarcts are black and associated with volume loss; note the enlargement of the sulci and occipital horn of the lateral ventricle.
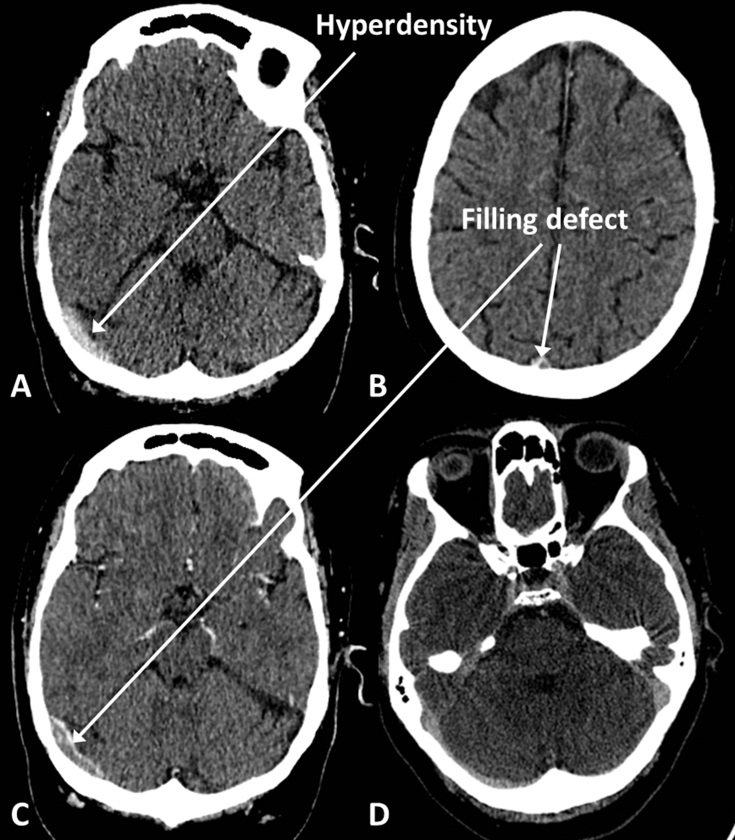
Venous sinus thrombosis. (A) Hyperdense clot in right transverse sinus on unenhanced CT. (B) Filling defect in superior sagittal sinus on CT venogram (CTV). (C) Filling defect in right transverse sinus on CTV. (D) Normal CTV for comparison; notice that the sinuses should opacify homogenously.
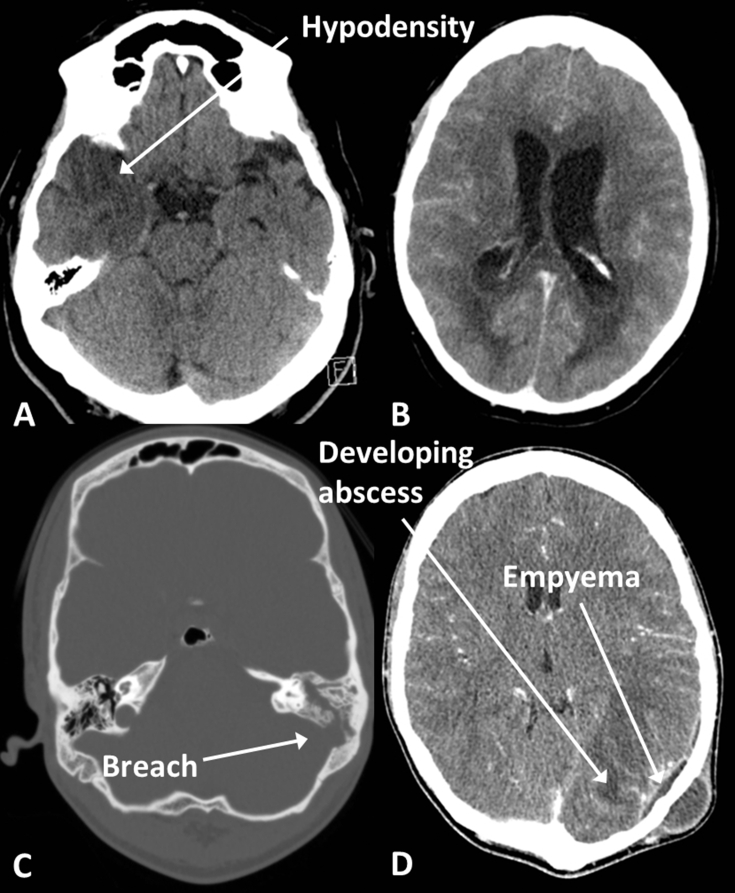
Infection. (A) Herpes encephalitis, with low density in the right temporal lobe. (B) Ventriculitis in a different patient; note the enhancement of the ventricle walls and the fluid levels in the occipital horns. (C) Mastoiditis with fluid in the left mastoid air cells (compare with the aerated right mastoid air cells) and a breach in the bony wall of the mastoid. (D) Empyema and abscess in the same patient as (C) secondary to the mastoid infection; note also the scalp abscess.
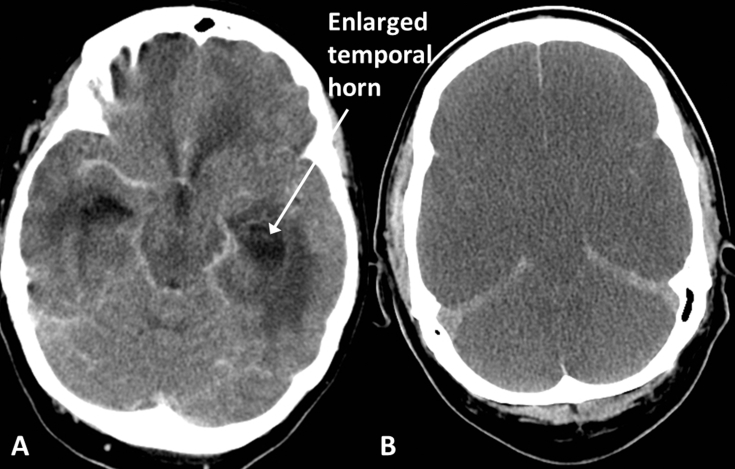
(A) Hydrocephalus, in a patient with ventriculitis; note the enlarged temporal horns and surrounding low density oedema. (B) Diffuse hypoxic brain injury; note the diffuse loss of grey/white differentiation and generalised swelling causing effacement of the sulci and cisterns in this patient after an out-of-hospital cardiac arrest. There is no haemorrhage but the tentorium and falx appear dense relative to the adjacent hypodense oedematous brain.

Tumours. (A) Metastases, hyperdense lesion in left basal ganglia and right frontal oedema related to a second lesion; (B) high-grade glioma, large heterogenous mass containing areas of haemorrhage and enhancement, crossing the corpus callosum; and (C) lymphoma, uniformly enhancing periventricular mass.
References
-
- Whiting P., Singatullina N., Rosser J. Computed tomography of the chest: I. Basic principles. Br J Anaesth Educ. 2015;15:299–304.
-
- American College of Radiology, American Society of Neuroradiology and Society for Paediatric Radiology . ACR, ASNR & SPR; 2015. Practice parameter for the performance of computed tomography (CT) of the brain.https://www.acr.org/-/media/ACR/Files/Practice-Parameters/CT-Brain.pdf Available from:
-
- National Institue for Health and Care Excellence . NICE Guideline (CG176); 2014. Head injury: assessment and early management.https://www.nice.org.uk/guidance/cg176 Available from: - PubMed
-
- Hofmeijer J., Kappelle L.J., Algra A., Amelink G.J., van Gijn J., van der Worp H.B., HAMLET investigators Surgical decompression for space-occupying cerebral infarction (the Hemicraniectomy After Middle Cerebral Artery infarction with Life-threatening Edema Trial [HAMLET]): a multicentre, open randomised trial. Lancet Neurol. 2009;8:326–333. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
