

Review
doi: 10.1016/j.bjae.2019.03.003.
Epub 2019 Apr 24.
Perioperative point-of-care gastric ultrasound
Affiliations
- PMID: 33456894
- PMCID: PMC7808010
- DOI: 10.1016/j.bjae.2019.03.003
Item in Clipboard
Review
Perioperative point-of-care gastric ultrasound
BJA Educ.
2019 Jul.
No abstract available
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

Graphical representation of the different gastric sections. A representative cross-section of the five layers of the gastric antrum that can be seen sonographically is demonstrated on the right.
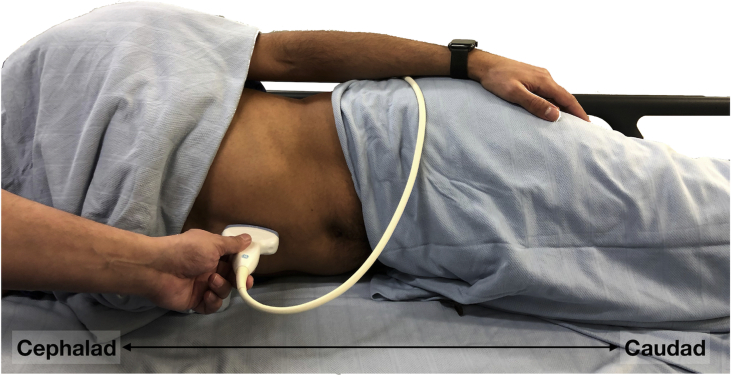
Patient positioning for performing gastric ultrasound in the RLD position, with the ultrasound transducer placed in the epigastrium beneath the xiphoid process.

Ultrasound images of an empty gastric antrum, with the key sonographic landmarks identified on the right. SMA, superior mesenteric artery.

Ultrasound images of different antral qualitative appearances. (A) Gastric antrum (A) containing fluid with some air bubbles. (B) Gastric antrum containing fluid with a ‘starry night’ appearance. Antral CSA was calculated with a calliper trace tool (yellow dotted line), and a CSA of 27.34 cm2 was quantified. (C) Gastric antrum after recent ingestion of solids, with a ‘frosted glass’ appearance. The anterior antral wall is visible, but there are no clear structures seen deep to the anterior antral wall. (D) Gastric antrum containing solids, with heterogeneous echogenicity representing different consistency of solids consumed. Note the thin, hypoechoic muscularis propriae compared to Fig 3. SMA, superior mesenteric artery.
References
-
- Engelhardt T., Webster N.R. Pulmonary aspiration of gastric contents in anaesthesia. Br J Anaesth. 1999;83:453–460. - PubMed
-
- Van De Putte P., Vernieuwe L., Jerjir A., Verschueren L., Tacken M., Perlas A. When fasted is not empty: a retrospective cohort study of gastric content in fasted surgical patients. Br J Anaesth. 2017;118:363–371. - PubMed
-
- Perlas A., Chan V.W.S., Lupu C.M., Mitsakakis N., Hanbidge A. Ultrasound assessment of gastric content and volume. Anesthesiology. 2009;111:82–89. - PubMed
-
- Perlas A., Mitsakakis N., Liu L. Validation of a mathematical model for ultrasound assessment of gastric volume by gastroscopic examination. Anesth Analg. 2013;116:357–363. - PubMed
-
- Van De Putte P., Perlas A. Ultrasound assessment of gastric content and volume. Br J Anaesth. 2014;113:12–22. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
