

Review
doi: 10.1016/j.bjae.2020.07.001.
Epub 2020 Aug 27.
Anaesthesia for lung transplantation
Affiliations
- PMID: 33456920
- PMCID: PMC7808022
- DOI: 10.1016/j.bjae.2020.07.001
Item in Clipboard
Review
Anaesthesia for lung transplantation
BJA Educ.
2020 Nov.
No abstract available
Keywords: anaesthesia; lung; transplantation.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
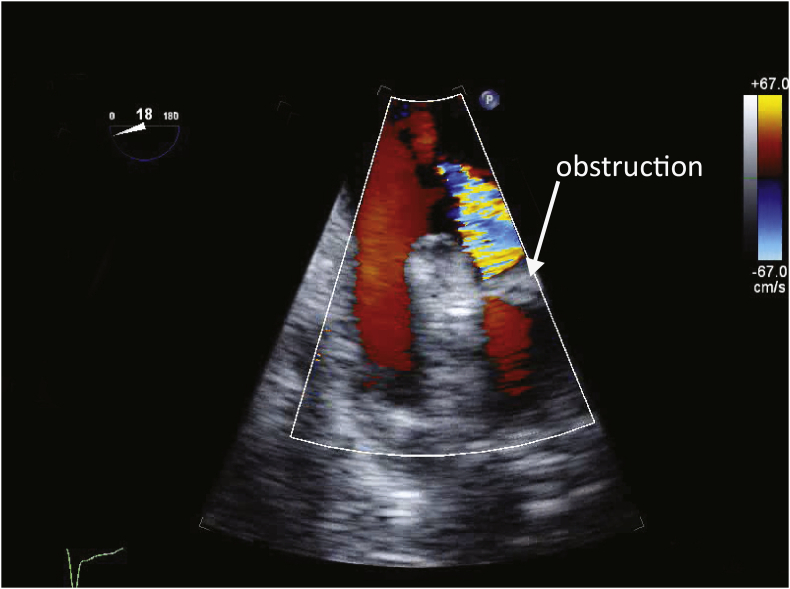
Pulmonary venous obstruction. The image shows a transoesophageal echocardiography (TOE) view of the left-sided pulmonary veins after allograft reperfusion. An obstruction can be seen in one of the veins, possibly caused by torsion of the lung. With colour Doppler imaging, aliased, high-velocity flow is seen proximal to the obstruction. In contrast, flow in the other vein is laminar and of low velocity.

Right ventricular dysfunction. In this mid-oesophageal four-chamber transoesophageal echocardiography (TOE) view obtained during diastole, marked dilatation of the right atrium (RA) and ventricle (RV) can be seen. The atrial and ventricular septa are displaced leftward. The left atrium (LA) and ventricle (LV) are reduced in size compared with normal. These findings are typical of severe right ventricular volume overload. Not evident in this still frame, but obvious with real-time imaging, is severe RV systolic dysfunction.

Primary graft dysfunction. The image shows a chest radiograph from a patient who underwent lung transplantation 2 days earlier. The patient developed primary graft dysfunction requiring VV ECMO. Diffuse alveolar opacities are present throughout both lungs. The tips of the drainage and return ECMO cannulae are demonstrated. Other identifiable features include a tracheal tube (the tip is positioned at the origin of the right main bronchus and needs to be withdrawn slightly), four chest drains, two external defibrillator pads, a sternal wire at the base of the sternum (a characteristic finding after a ‘clamshell’ incision), and a small amount of subcutaneous air in the chest wall adjacent to the base of the left lung. VV ECMO, venovenous extracorporeal membrane oxygenation.
References
-
- Chambers D.C., Cherikh W.S., Harhay M.O. The international thoracic organ transplant registry of the international society for heart and lung transplantation: thirty-sixth adult lung and heart–lung transplantation report—2019; focus theme: donor and recipient size match. J Heart Lung Transplant. 2019;38:1042–1055. - PMC - PubMed
-
- Conor S. Statistica.com. Lung transplants in the United Kingdom (UK) 2018/2019. Available from: https://www.statista.com/statistics/518774/number-of-lung-transplants-un... (Accessed 14 April 2020).
-
- Weill D., Benden C., Corris P.A. A consensus document for the selection of lung transplant candidates: 2014—an update from the pulmonary transplantation council of the international society for heart and lung transplantation. J Heart Lung Transplant. 2015;34:1–15. - PubMed
-
- Martin A.K., Renew J.R., Jayaraman A.L., Murray A.W., Fritz A.V., Ramakrishna H. Analysis of outcomes in lung transplantation. J Cardiothorac Vasc Anesth. 2019;33:1455–1466. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
