

Nurse-Led Call Back Program to Improve Patient Follow-Up With Providers After Discharge From the Emergency Department
- PMID: 33457586
- PMCID: PMC7786663
- DOI: 10.1177/2374373520947925
Nurse-Led Call Back Program to Improve Patient Follow-Up With Providers After Discharge From the Emergency Department
Abstract
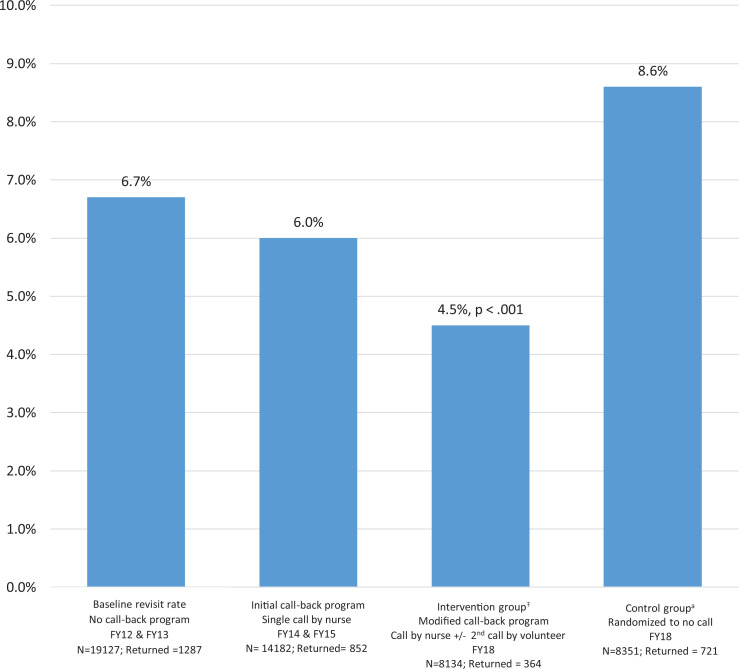
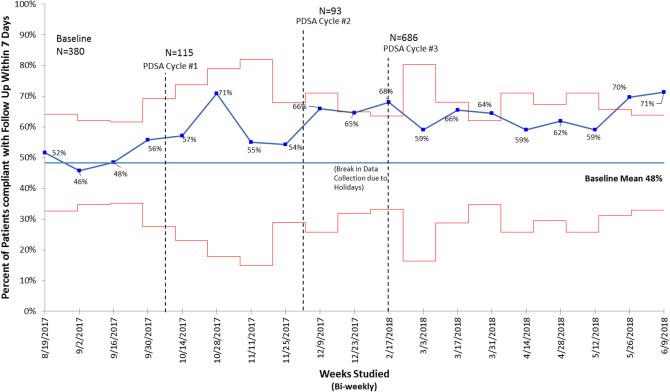
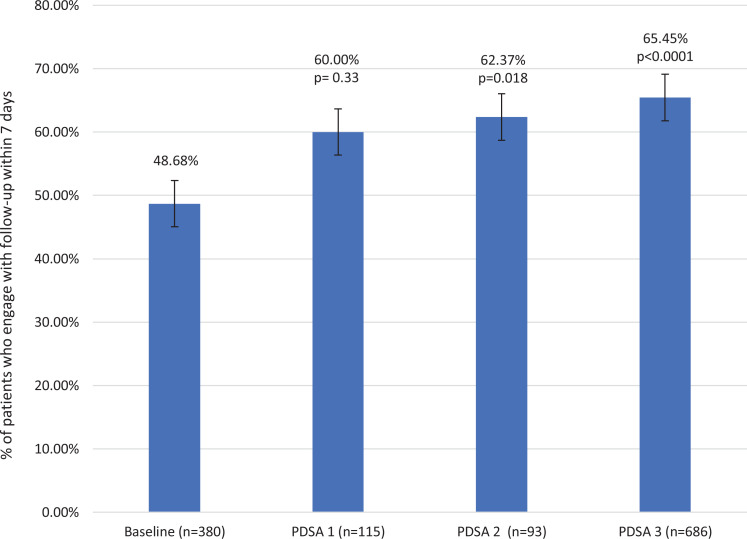
Phone calls to patients after discharge from the emergency department (ED) serve as reminders to schedule medical follow-up, support adherence to discharge instructions, and reduce revisits to already-crowded EDs. An existing, nurse-administered, call-back program contacted randomly selected ED patients 24 to 48 hours following discharge. This program did not improve patient follow-up (48.68%) nor reduce the ED revisit rate (6.7% baseline vs 6.0% postimplementation). Plan-Do-Study-Act methodology tested a modification to the existing program consisting of a second, scripted phone call from a trained volunteer at 72 to 96 hours postdischarge. Volunteers utilized a patient list and script, and nurses provided expertise to eliminate identified barriers to follow-up. Follow-up rate and ED revisit were monitored through the electronic medical record. A total of 894 patients participated between October 2017 and June 2018. Follow-up increased from 48.68% to 65.5% (P < .0001) and ED revisit decreased significantly (4.5% vs 8.6%, P < .001). This innovative nurse-led, systematic postdischarge call-back program utilizing hospital volunteers increased patient compliance with post-ED medical follow-up while significantly reducing the rate of patient revisit to the ED within 7 days of discharge.
Keywords: clinician–patient relationship; communication; nursing; patient engagement; patient feedback; quality improvement; transitions of care.
© The Author(s) 2020.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Hooker EA, Mallow PJ, Oglesby MM. Characteristics and trends of emergency department visits in the United States (2010-2014). J Emerg Med. 2019;56:344–351. - PubMed
-
- Moskop JC, Geiderman JM, Marshall KD, McGreevy J, Derse AR, Bookman K, et al. Another look at the persistent moral problem of emergency department crowding. Ann Emerg Med. 2019;74:357–364. - PubMed
-
- Duseja R, Bardach NS, Lin GA, Yazdany J, Dean ML, Clay TH, et al. Revisit rates and associated costs after an emergency department encounter: a multistate analysis. Ann Intern Med. 2015;162:750–756. - PubMed
-
- Crocker JB, Crocker JT, Greenwald JL. Telephone follow-up as a primary care intervention for postdischarge outcomes improvement: a systematic review. Am J Med. 2012;125:915–921. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
