

Antegrade and Retrograde Endoscopic Approaches for Managing Obstructing Ureteral Calculi in Renal Transplant Patients: An Illustrative Case Series
- PMID: 33457671
- PMCID: PMC7803235
- DOI: 10.1089/cren.2020.0063
Antegrade and Retrograde Endoscopic Approaches for Managing Obstructing Ureteral Calculi in Renal Transplant Patients: An Illustrative Case Series
Abstract
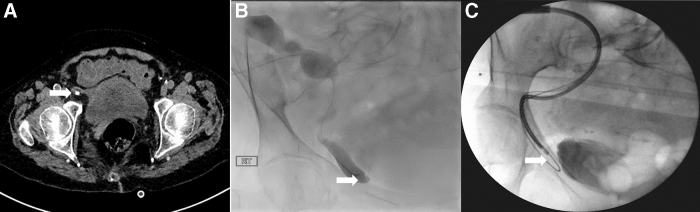
Purpose: To demonstrate the various antegrade and retrograde endourologic approaches that may be required for effectively treating kidney transplant recipients presenting with ureteral obstruction caused by urolithiasis. Materials and Methods: We prospectively evaluated endoscopic management techniques of renal transplant recipients referred to a national kidney transplant center with obstructing transplant ureteral calculi for a 12-month period (April 2019-April 2020). Results: Four kidney transplant recipients presented with ureteral obstruction caused by urolithiasis and the mean age was 66.6 (range: 62-71) years. The mean duration from renal transplantation was 16 (range: 6-25) years. Three patients presented with acute urosepsis and one patient presented with malaise and recurrent urinary tract infections. Two patients were definitively treated with percutaneous antegrade flexible ureteroscopic lithotripsy through a 16F minipercutaneous nephrolithotomy sheath. Two patients were definitively treated with retrograde flexible ureteroscopy (7F single-use disposable ureteroscope) and laser lithotripsy. Full stone clearance was achieved in all four patients and no perioperative complications occurred. Conclusion: Management of ureteral calculi in renal transplant recipients is challenging. A multimodal approach involving antegrade and retrograde endoscopic techniques may be required to achieve full stone clearance.
Keywords: kidney transplant; urinary tract calculi; urinary tract calculi in transplant ureters; urolithiasis.
Copyright 2020, Mary Ann Liebert, Inc., publishers.
Conflict of interest statement
No competing financial interests exist.
Figures



Similar articles
-
Ureteropyeloscopic treatment of large, complex intrarenal and proximal ureteral calculi.BJU Int. 2013 Mar;111(3 Pt B):E127-31. doi: 10.1111/j.1464-410X.2012.11352.x. Epub 2012 Jul 3. BJU Int. 2013. PMID: 22757752
-
Retrograde ureteropyeloscopic treatment of 2 cm. or greater upper urinary tract and minor Staghorn calculi.J Urol. 1998 Aug;160(2):346-51. J Urol. 1998. PMID: 9679874
-
Multimodal management of urolithiasis in renal transplantation.BJU Int. 2005 Aug;96(3):385-9. doi: 10.1111/j.1464-410X.2005.05636.x. BJU Int. 2005. PMID: 16042735
-
Combined treatment of ureteropelvic junction obstruction and renal calculi with robot-assisted laparoscopic pyeloplasty and laser lithotripsy in children: Case report and non-systematic review of the literature.Int J Med Robot. 2021 Jun;17(3):e2246. doi: 10.1002/rcs.2246. Epub 2021 Mar 7. Int J Med Robot. 2021. PMID: 33626232 Review.
-
[Endoscopic techniques in the treatment of calculi in the upper urinary tract].Tidsskr Nor Laegeforen. 1996 Oct 10;116(24):2893-6. Tidsskr Nor Laegeforen. 1996. PMID: 8975406 Review. Norwegian.
Cited by
-
DIFFERENT APPROACHES TO MANAGING UROLITHIASIS IN KIDNEY TRANSPLANT PATIENTS - A CASE REPORT.Acta Clin Croat. 2023 Jul;62(Suppl2):132-137. doi: 10.20471/acc.2023.62.s2.19. Acta Clin Croat. 2023. PMID: 38966036 Free PMC article.
References
-
- Stravodimos KG, Adamis S, Tyritzis S, Georgios Z, Constantinides CA. Renal transplant lithiasis: Analysis of our series and review of the literature. J Endourol 2012;26:38–44 - PubMed
-
- Basiri A, Nikoobakht MR, Simforoosh N, Hosseini Moghaddam SM. Ureteroscopic management of urological complications after renal transplantation. Scand J Urol nephrol 2006;40:53–56 - PubMed
-
- He Z, Li X, Chen L, Zeng G, Yuan J. Minimally invasive percutaneous nephrolithotomy for upper urinary tract calculi in transplanted kidneys. BJU Int 2007;99:1467–1471 - PubMed
-
- Considine SW, Davis NF, McLoughlin LC, et al. . Long-term outcomes of en-bloc renal transplantation from paediatric donors into adult recipients. Surgeon 2019;17:1–5 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous