

Analytical modeling of depth-dose degradation in heterogeneous lung tissue for intensity-modulated proton therapy planning
- PMID: 33458311
- PMCID: PMC7807882
- DOI: 10.1016/j.phro.2020.05.001
Analytical modeling of depth-dose degradation in heterogeneous lung tissue for intensity-modulated proton therapy planning
Abstract
Background and purpose: Proton therapy may be promising for treating non-small-cell lung cancer due to lower doses to the lung and heart, as compared to photon therapy. A reported challenge is degradation, i.e., a smoothing of the depth-dose distribution due to heterogeneous lung tissue. For pencil beams, this causes a distal falloff widening and a peak-to-plateau ratio decrease, not considered in clinical treatment planning systems.
Materials and methods: We present a degradation model implemented into an analytical dose calculation, fully integrated into a treatment planning workflow. Degradation effects were investigated on target dose, distal dose falloffs, and mean lung dose for ten patient cases with varying anatomical characteristics.
Results: For patients with pronounced range straggling (in our study large tumors, or lesions close to the mediastinum), degradation effects were restricted to a maximum decrease in target coverage (D 95 of the planning target volume) of 1.4%. The median broadening of the distal 80-20% dose falloffs was 0.5 mm at the maximum. For small target volumes deep inside lung tissue, however, the target underdose increased considerably by up to 26%. The mean lung dose was not negatively affected by degradation in any of the investigated cases.
Conclusion: For most cases, dose degradation due to heterogeneous lung tissue did not yield critical organ at risk overdosing or overall target underdosing. However, for small and deep-seated tumors which can only be reached by penetrating lung tissue, we have seen substantial local underdose, which deserves further investigation, also considering other prevalent sources of uncertainty.
Keywords: Bragg peak degradation; Depth-dose degradation; Heterogeneous lung tissue; Non-small-cell lung carcinoma; Proton therapy; Radiotherapy planning.
© 2020 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
On the Way to Accounting for Lung Modulation Effects in Particle Therapy of Lung Cancer Patients-A Review.Cancers (Basel). 2024 Oct 25;16(21):3598. doi: 10.3390/cancers16213598. Cancers (Basel). 2024. PMID: 39518037 Free PMC article. Review.
-
Effects of the Bragg peak degradation due to lung tissue in proton therapy of lung cancer patients.Radiat Oncol. 2019 Oct 25;14(1):183. doi: 10.1186/s13014-019-1375-0. Radiat Oncol. 2019. PMID: 31653229 Free PMC article.
-
Quantification of the dependencies of the Bragg peak degradation due to lung tissue in proton therapy on a CT-based lung tumor phantom.Phys Med Biol. 2019 Aug 1;64(15):155005. doi: 10.1088/1361-6560/ab2611. Phys Med Biol. 2019. PMID: 31151126
-
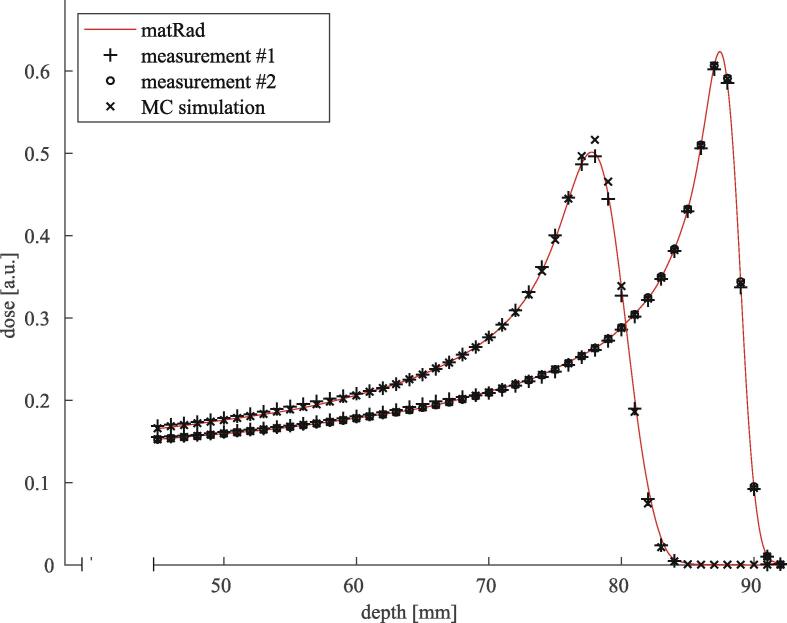
Investigation of the Bragg peak degradation caused by homogeneous and heterogeneous lung tissue substitutes: proton beam experiments and comparison to current clinical dose calculation.Phys Med Biol. 2020 Dec 11;65(24). doi: 10.1088/1361-6560/abc938. Phys Med Biol. 2020. PMID: 33171454
-
Recent advances in light ion radiation therapy.Int J Radiat Oncol Biol Phys. 2004 Feb 1;58(2):603-16. doi: 10.1016/j.ijrobp.2003.09.034. Int J Radiat Oncol Biol Phys. 2004. PMID: 14751534 Review.
Cited by
-
On the Way to Accounting for Lung Modulation Effects in Particle Therapy of Lung Cancer Patients-A Review.Cancers (Basel). 2024 Oct 25;16(21):3598. doi: 10.3390/cancers16213598. Cancers (Basel). 2024. PMID: 39518037 Free PMC article. Review.
References
-
- Zschaeck S., Simon M., Löck S., Troost E.G.C., Stützer K., Wohlfahrt P. PRONTOX – proton therapy to reduce acute normal tissue toxicity in locally advanced non-small-cell lung carcinomas (NSCLC): study protocol for a randomised controlled trial. Trials. 2016;17:543. doi: 10.1186/s13063-016-1679-4. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
