

Evaluation of an a priori scatter correction algorithm for cone-beam computed tomography based range and dose calculations in proton therapy
- PMID: 33458349
- PMCID: PMC7807858
- DOI: 10.1016/j.phro.2020.09.014
Evaluation of an a priori scatter correction algorithm for cone-beam computed tomography based range and dose calculations in proton therapy
Abstract
Background and purpose: Scatter correction of cone-beam computed tomography (CBCT) projections may enable accurate online dose-delivery estimations in photon and proton-based radiotherapy. This study aimed to evaluate the impact of scatter correction in CBCT-based proton range/dose calculations, in scans acquired in both proton and photon gantries.
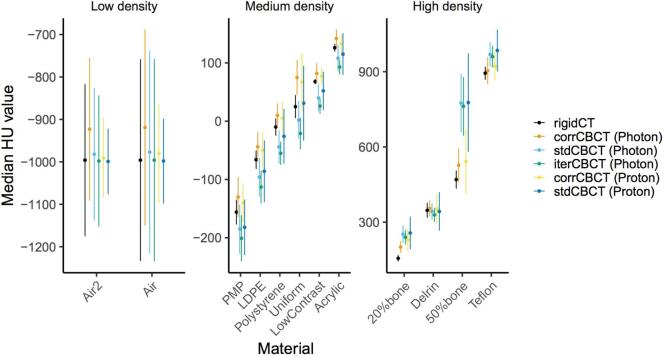
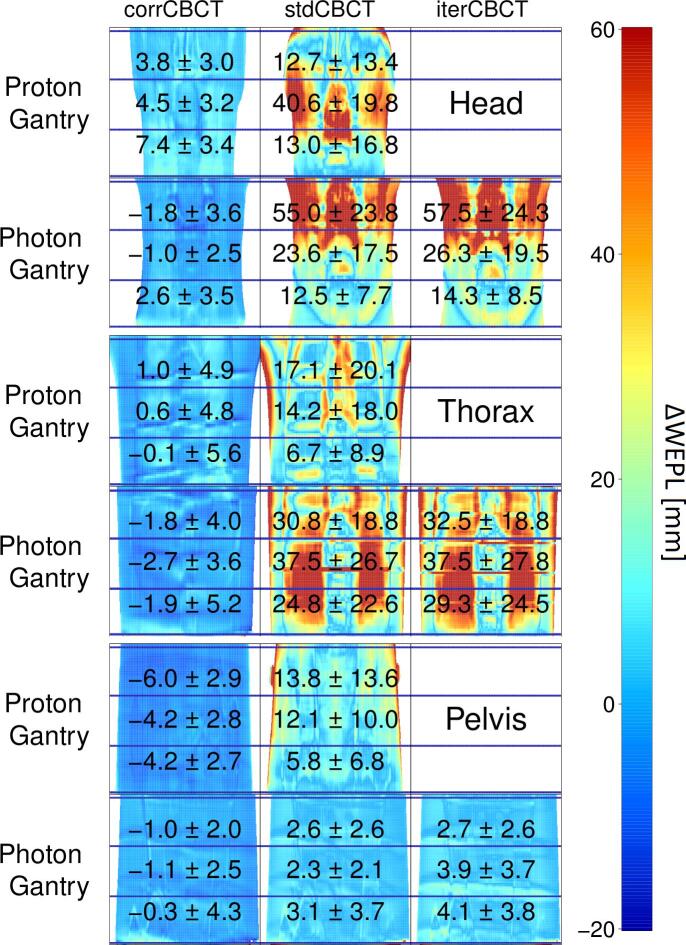
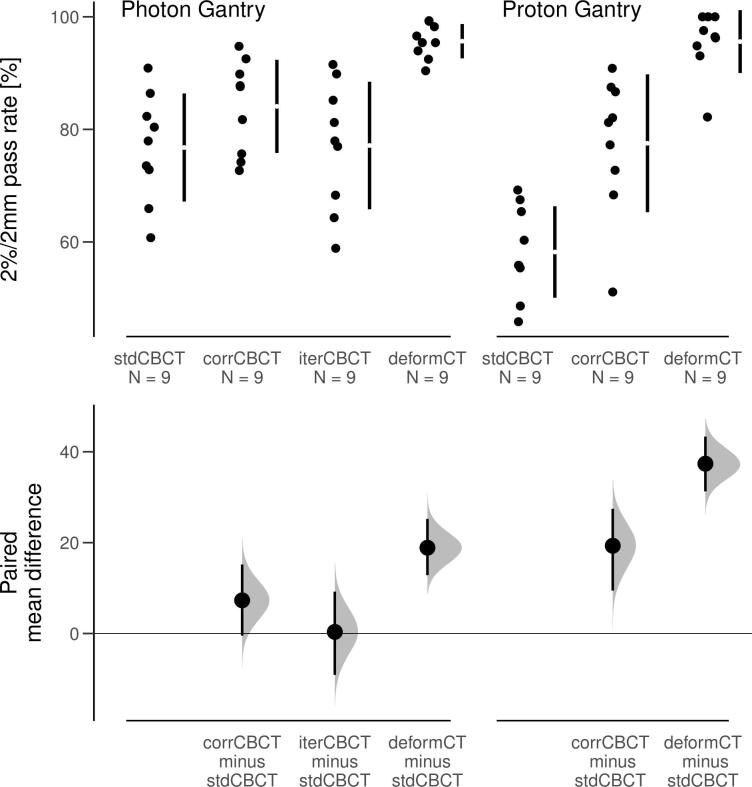
Material and methods: CBCT projections of a Catphan and an Alderson phantom were acquired on both a proton and a photon gantry. The scatter corrected CBCTs (corrCBCTs) and the clinical reconstructions (stdCBCTs) were compared against CTs rigidly registered to the CBCTs (rigidCTs). The CBCTs of the Catphan phantom were segmented by materials for CT number analysis. Water equivalent path length (WEPL) maps were calculated through the Alderson phantom while proton plans optimized on the rigidCT and recalculated on all CBCTs were compared in a gamma analysis.
Results: In medium and high-density materials, the corrCBCT CT numbers were much closer to those of the rigidCT than the stdCBCTs. E.g. in the 50% bone segmentations the differences were reduced from above 300 HU (with stdCBCT) to around 60-70 HU (with corrCBCT). Differences in WEPL from the rigidCT were typically well below 5 mm for the corrCBCTs, compared to well above 10 mm for the stdCBCTs with the largest deviations in the head and thorax regions. Gamma pass rates (2%/2mm) when comparing CBCT-based dose re-calculations to rigidCT calculations were improved from around 80% (with stdCBCT) to mostly above 90% (with corrCBCT).
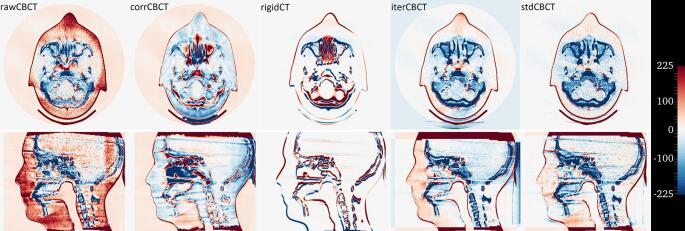
Conclusion: Scatter correction leads to substantial artefact reductions, improving accuracy of CBCT-based proton range/dose calculations.
Keywords: A priori; APT; Adaptive proton therapy; Beam hardening; CB; CBCT; Cone beam; Cone beam computed tomography; Cone beam projections; Dose calculation; Dose recalculation; Inter-fractional motion management; Projections; Proton; Range; Scatter; Scatter correction; Shading correction; WEPL; Water equivalent path length.
© 2020 The Authors. Published by Elsevier B.V. on behalf of European Society of Radiotherapy & Oncology.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

References
LinkOut - more resources
Full Text Sources
Research Materials
