

Stereotactic body proton therapy for liver tumors: Dosimetric advantages and their radiobiological and clinical implications
- PMID: 33458411
- PMCID: PMC7807648
- DOI: 10.1016/j.phro.2018.11.004
Stereotactic body proton therapy for liver tumors: Dosimetric advantages and their radiobiological and clinical implications
Abstract
Background and purpose: Photon Stereotactic Body Radiotherapy (SBRT) for primary and metastatic tumors of the liver is challenging for larger lesions. An in silico comparison of paired SBRT and Stereotactic Body Proton Therapy (SBPT) plans was performed to understand the potential advantages of SBPT as a function of tumor size and location.
Methods and materials: Theoretical tumor volumes with maximum diameter of 1-10 cm were contoured in the dome, right inferior, left medial, and central locations. SBRT and SBPT plans were generated to deliver 50 Gy in 5 fractions, max dose <135%. When organs-at-risk (OAR) constraints were exceeded, hypothetical plans (not clinically acceptable) were generated for comparison. Liver normal tissue complication probability (NTCP) models were applied to evaluate differences between treatment modalities.
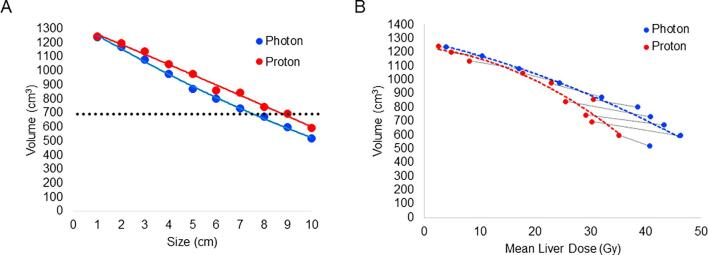
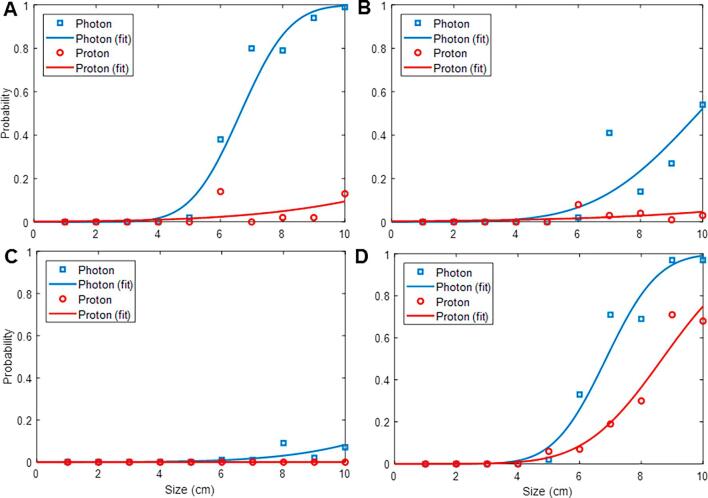
Results: SBRT and SBPT were able to meet target goals and OAR constraints for lesions up to 7 cm and 9 cm diameter, respectively. SBPT plans resulted in a higher integral gross target dose for all lesions up to 7 cm (mean dose 57.8 ± 2.3 Gy to 64.1 ± 2.2 Gy, p < 0.01). Simultaneously, SBPT spared dose to the uninvolved liver in all locations (from 11.5 ± 5.3 Gy to 8.6 ± 4.4 Gy, p < 0.01), resulting in lower NTCP particularly for larger targets in the dome and central locations. SBPT also spared duodenal dose across all sizes and positions (from 7.3 ± 1.1 Gy to 1.1 ± 0.3 Gy, p < 0.05).
Conclusion: The main advantages of SBPT over SBRT is meeting plan goals and constrains for larger targets, particularly dome and central locations, and sparing dose to uninvolved liver. For such patients, SBPT may allow improvements in tumor control and treatment safety.
Keywords: Liver SBRT; NTCP; Proton SBRT.
© 2018 The Authors.
Figures
References
-
- Bujold A., Massey C.A., Kim J.J., Brierley J., Cho C., Wong R.K. Sequential phase I and II trials of stereotactic body radiotherapy for locally advanced hepatocellular carcinoma. J Clin Oncol. 2013;31:1631–1639. - PubMed
-
- Barry A., McPartlin A., Lindsay P., Wang L., Brierley J., Kim J. Dosimetric analysis of liver toxicity after liver metastasis stereotactic body radiation therapy. Pract Radiat Oncol. 2017 - PubMed
-
- Swaminath A., Massey C., Brierley J.D., Dinniwell R., Wong R., Kim J.J. Accumulated Delivered Dose Response of Stereotactic Body Radiation Therapy for Liver Metastases. Int J Radiat Oncol Biol Phys. 2015;93:639–648. - PubMed
-
- Sapisochin G., Barry A., Doherty M., Fischer S., Goldaracena N., Rosales R. Stereotactic body radiotherapy vs. TACE or RFA as a bridge to transplant in patients with hepatocellular carcinoma. An intention-to-treat analysis. J Hepatol. 2017;67:92–99. - PubMed
-
- Hong J.C., Salama J.K. The expanding role of stereotactic body radiation therapy in oligometastatic solid tumors: What do we know and where are we going? Cancer Treat Rev. 2017;52:22–32. - PubMed
LinkOut - more resources
Full Text Sources
