

Clinical implementation of magnetic resonance imaging guided adaptive radiotherapy for localized prostate cancer
- PMID: 33458428
- PMCID: PMC7807673
- DOI: 10.1016/j.phro.2019.02.002
Clinical implementation of magnetic resonance imaging guided adaptive radiotherapy for localized prostate cancer
Abstract
Background and purpose: Magnetic resonance-guided radiation therapy (MRgRT) has recently become available in clinical practice and is expected to expand significantly in coming years. MRgRT offers marker-less continuous imaging during treatment delivery, use of small clinical target volume (CTV) to planning target volume (PTV) margins, and finally the option to perform daily plan re-optimization.
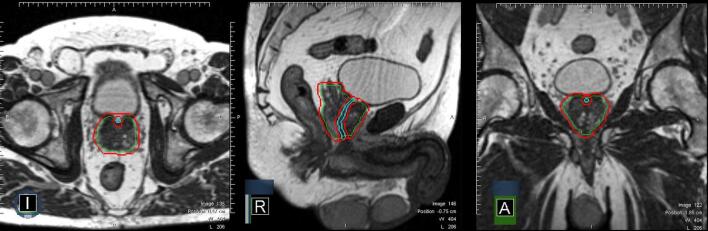
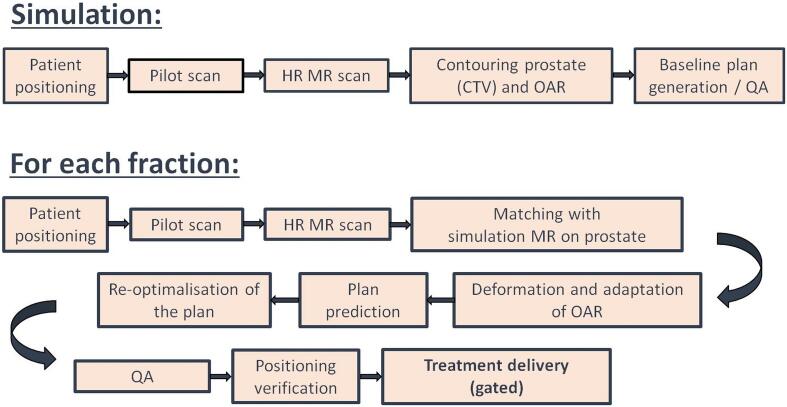
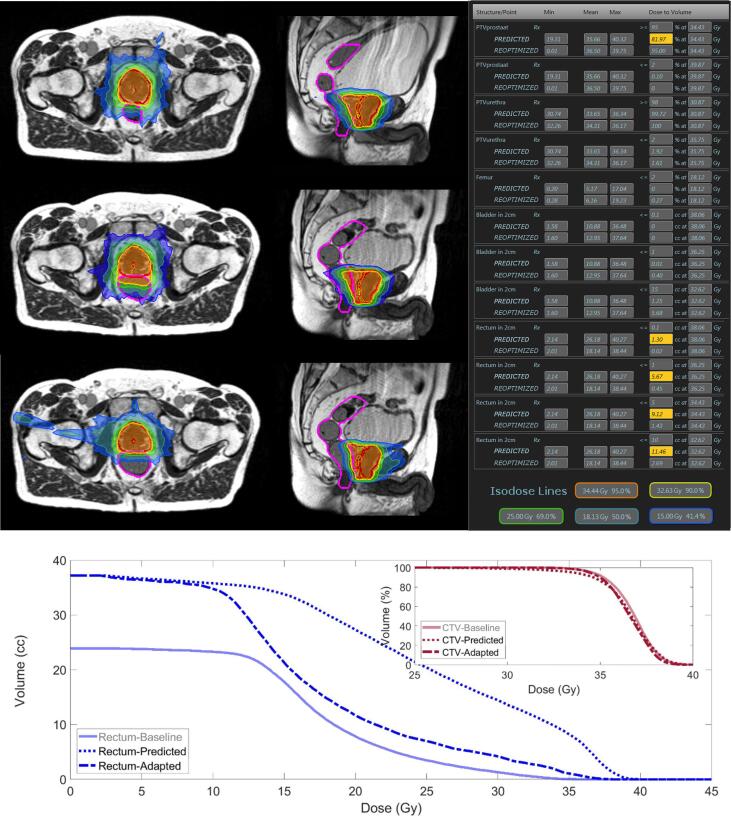
Materials and methods: A total of 140 patients (700 fractions) have been treated with MRgRT and online plan adaptation for localized prostate cancer since early 2016. Clinical workflow for MRgRT of prostate cancer consisted of patient selection, simulation on both MR- and computed tomography (CT) scan, inverse intensity-modulated radiotherapy (IMRT) treatment planning and daily plan re-optimization prior to treatment delivery with partial organs at risk (OAR) recontouring within the first 2 cm outside the PTV. For each adapted plan online patient-specific quality assurance (QA) was performed by means of a secondary Monte Carlo 3D dose calculation and gamma analysis comparison. Patient experiences with MRgRT were assessed using a patient-reported outcome questionnaire (PRO-Q) after the last fraction.
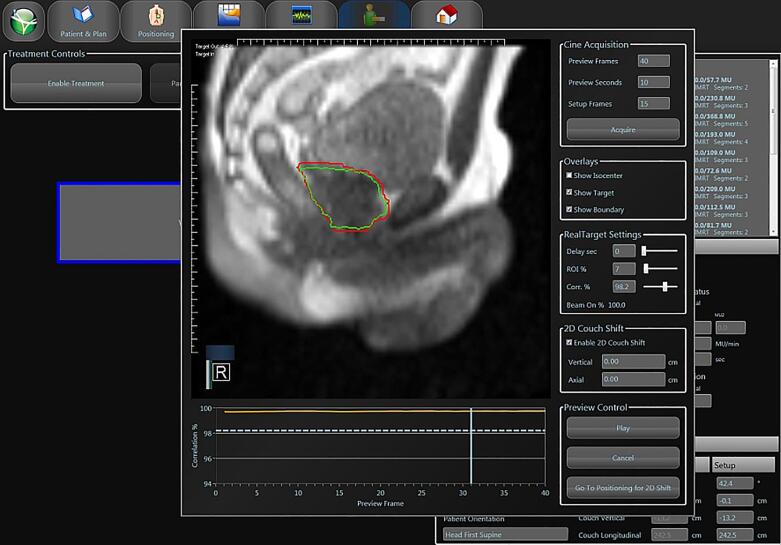
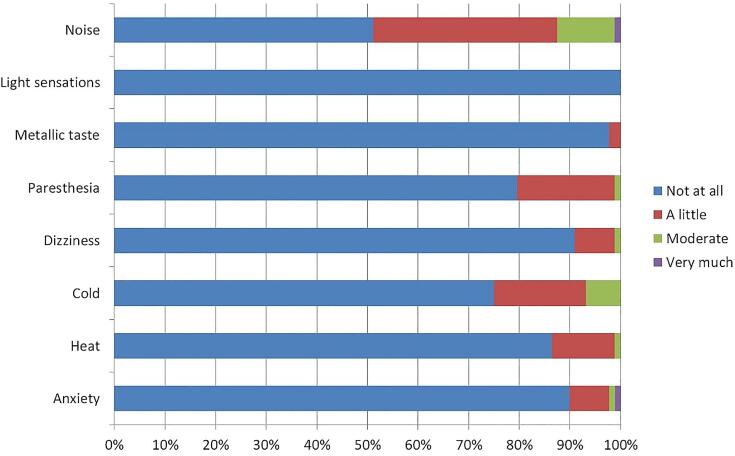
Results: In 97% of fractions, MRgRT was delivered using the online adapted plan. Intrafractional prostate drifts necessitated 2D-corrections during treatment in approximately 20% of fractions. The average duration of an uneventful fraction of MRgRT was 45 min. PRO-Q's (N = 89) showed that MRgRT was generally well tolerated, with disturbing noise sensations being most commonly reported.
Conclusions: MRgRT with daily online plan adaptation constitutes an innovative approach for delivering SBRT for prostate cancer and appears to be feasible, although necessitating extended timeslots and logistical challenges.
Keywords: MR-guided Radiotherapy (MRgRT); On-table adaptation; Prostate cancer; Stereotactic body radiotherapy (SBRT); Workflow.
© 2019 The Authors.
Figures
References
-
- Miralbell R., Roberts S.A., Zubizarreta E., Hendry J.H. Dose-fractionation sensitivity of prostate cancer deduced from radiotherapy outcomes of 5,969 patients in seven international institutional datasets: α/β = 1.4 (0.9-2.2) Gy. Int J Radiat Oncol Biol Phys. 2012;82:17–24. doi: 10.1016/j.ijrobp.2010.10.075. - DOI - PubMed
-
- Proust-Lima C., Taylor J.M.G., Sécher S., Sandler H., Kestin L., Pickles T. Confirmation of a low α/β ratio for prostate cancer treated by external beam radiation therapy alone using a post-treatment repeated-measures model for PSA dynamics. Int J Radiat Oncol Biol Phys. 2011;79:195–201. doi: 10.1016/j.ijrobp.2009.10.008. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
