

Ensuring Business Continuity of Musculoskeletal Care During the COVID-19 Pandemic: Experience of a Tertiary Orthopaedic Surgery Department in Singapore
- PMID: 33458559
- PMCID: PMC7592874
- DOI: 10.2106/JBJS.OA.20.00050
Ensuring Business Continuity of Musculoskeletal Care During the COVID-19 Pandemic: Experience of a Tertiary Orthopaedic Surgery Department in Singapore
Abstract
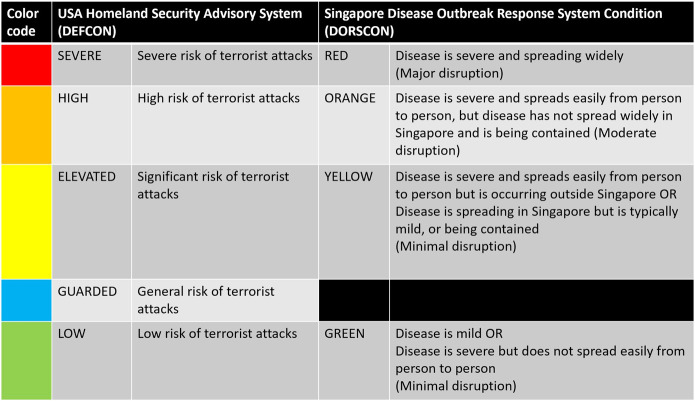
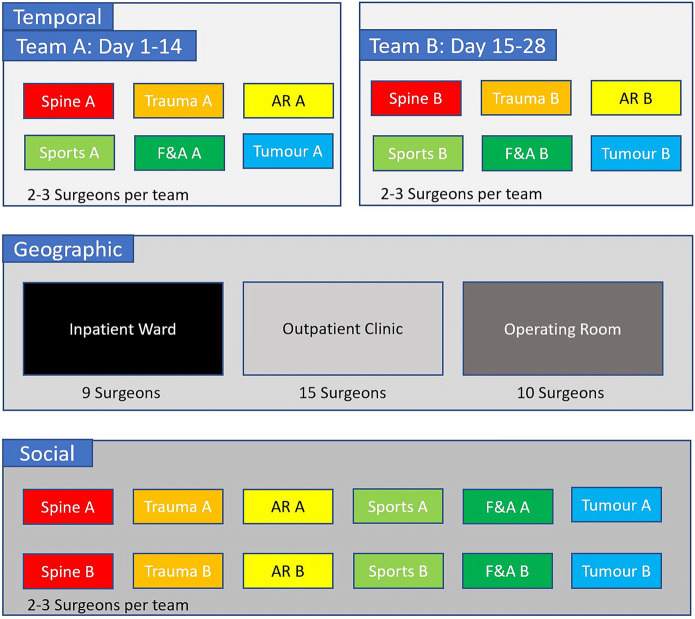
On February 8, 2020, Singapore raised its Disease Outbreak Response System Condition (DORSCON) level to Orange, indicating that coronavirus 2019 (COVID-19) was a severe disease with high human transmissibility. Using lessons learned from the severe acute respiratory syndrome (SARS) outbreak in 2003, the orthopaedic surgery department at Singapore General Hospital, a tertiary-level referral center, was prepared to handle this pandemic through business-continuity planning. The business that we are referring to is the "business" of orthopaedic surgery, encompassing clinical care, education, research, and administration. There is a lack of literature detailing business-continuity plans of surgical departments during pandemics, with new guidelines being developed. A large proportion of orthopaedic work, such as cases of fracture and infection, cannot be postponed. Even elective surgeries cannot be postponed indefinitely as it could result in detriment to the quality of life of patients. The aim of this article is to detail the business-continuity plans at our institution that allowed the delivery of essential musculoskeletal care through personnel segregation measures during the COVID-19 pandemic. Strategies to ensure the provision of timely medical intelligence, the reduction of nonessential ambulatory visits and surgical procedures, ensuring the safety and morale of staff, and continuing education and research efforts were paramount. As the COVID-19 pandemic unfolds, our posture needs to constantly evolve to meet new challenges that may come our way. Our existing business-continuity plan is not perfect and may not be applicable to smaller hospitals. There is conflict between envisioned normalcy, remaining economically viable as an orthopaedic department, and fulfilling training requirements, and educating the next generation of orthopaedic surgeons on the one hand and the need for segregation, workload reduction, virtual education, and social distancing on the other. Orthopaedic surgeons need to strike a balance between business continuity and adopting sustainable precautions against COVID-19. We hope that our experience will aid other orthopaedic surgery departments in adapting to this new norm, protecting their staff and patients, managing staff morale, and allowing the continuation of musculoskeletal care during the COVID-19 pandemic.
Copyright © 2020 The Authors. Published by The Journal of Bone and Joint Surgery, Incorporated. All rights reserved.
Conflict of interest statement
Disclosure: The authors indicated that no external funding was received for any aspect of this work. The Disclosure of Potential Conflicts of Interest forms are provided with the online version of the article (http://links.lww.com/JBJSOA/A167).
Figures
References
-
- Paules CI, Marston HD, Fauci AS. Coronavirus infections-more than just the common cold. JAMA. 2020. January 23. Epub 2020 Jan 23. - PubMed
-
- Adalja AA, Toner E, Inglesby TV. Priorities for the US health community responding to COVID-19. JAMA. 2020. March 3. Epub 2020 Mar 3. - PubMed
-
- Mahase E. Covid-19: WHO declares pandemic because of “alarming levels” of spread, severity, and inaction. BMJ. 2020. March 12;368:m1036. - PubMed
-
- Wong JEL, Leo YS, Tan CC. COVID-19 in Singapore-current experience: critical global issues that require attention and action. JAMA. 2020. February 20. Epub 2020 Feb 20. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous