

Extranodal Natural Killer/T-cell Lymphoma, Nasal Type: Diagnosis and Treatment
- PMID: 33458595
- PMCID: PMC7806244
- DOI: 10.1097/HS9.0000000000000523
Extranodal Natural Killer/T-cell Lymphoma, Nasal Type: Diagnosis and Treatment
Abstract
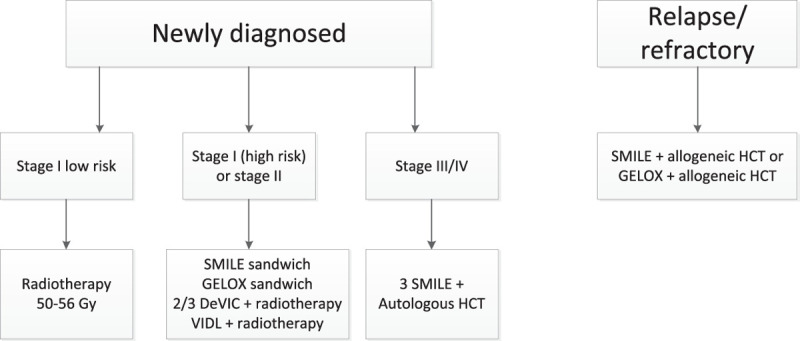
The aggressive lymphoma, extranodal natural killer/T-cell lymphoma-nasal type, is strongly associated with Epstein-Barr virus (EBV) and is most common in Asia and in South and Central America. By contrast, incidence is low in the United States and Europe, where extranodal natural killer/T-cell lymphoma represents only 0.2%-0.4% of all newly diagnosed non-Hodgkin lymphomas. At diagnosis, it is important to test for EBV DNA in plasma by polymerase chain reaction and to carry out positron emission tomography/computer tomography and magnetic resonance imaging of the nasopharynx. In stage I/II disease, radiotherapy is the most important treatment modality, but in high-risk stage I/II disease (stage II, age > 60 y, elevated lactate dehydrogenase, Eastern Cooperative Oncology Group performance score ≥2, primary tumor invasion), it should be combined with chemotherapy. The most optimal responses are reached with nonmultidrug resistance-based therapy (eg, asparaginase- or platinum-based therapy). Therapeutic approaches consist of either platinum-based concurrent chemoradiotherapy or sequential chemoradiotherapy. The minimum dose of radiotherapy should be 50-56 Gy. Treatment of stage III/IV disease consists of 3 cycles of chemotherapy followed by autologous hematopoietic cell transplantation. Allogeneic hematopoietic cell transplantation should only be considered in case of relapsed disease or after difficulty reaching complete remission. During treatment and follow-up, plasma EBV levels should be monitored as a marker of tumor load.
Copyright © 2021 the Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the European Hematology Association.
Conflict of interest statement
The authors declare no competing interest.
Figures

References
-
- van Doesum JA, Nijland M, Brink M, Huls GA, van Meerten T. A West-European cohort of patients with NK/T-cell lymphoma, a population-based analysis. HemaSphere. 2020; 4S1EP1238
-
- Karkera AC, Marshall Parson B, Borgert A, Go RS. NK/T cell lymphoma in the U.S.: a population-based study using the national cancer database from 1998-2012. J Clin Oncol. 2016; 3415_supple19038
-
- Tse E, Kwong YL. How I treat NK/T-cell lymphomas. Blood. 2013; 121:4997–5005 - PubMed
-
- Yang Y, Zhu Y, Cao JZ, et al. . Risk-adapted therapy for early-stage extranodal nasal-type NK/T-cell lymphoma: analysis from a multicenter study. Blood. 2015; 126:1424–1432; quiz 1517 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources