

Practical recommendations for timely, accurate diagnosis of symptomatic Alzheimer's disease (MCI and dementia) in primary care: a review and synthesis
- PMID: 33458891
- PMCID: PMC8359937
- DOI: 10.1111/joim.13244
Practical recommendations for timely, accurate diagnosis of symptomatic Alzheimer's disease (MCI and dementia) in primary care: a review and synthesis
Abstract
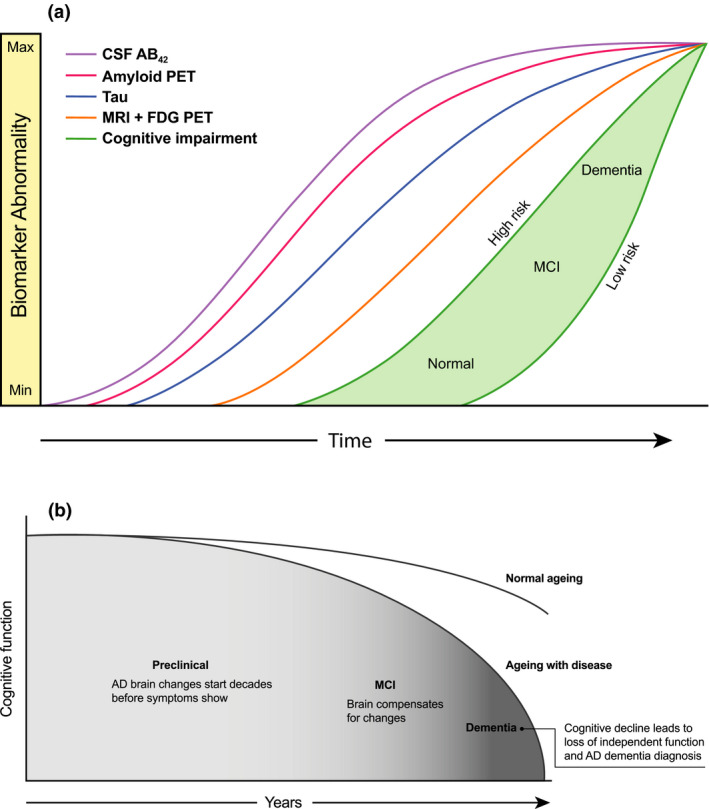
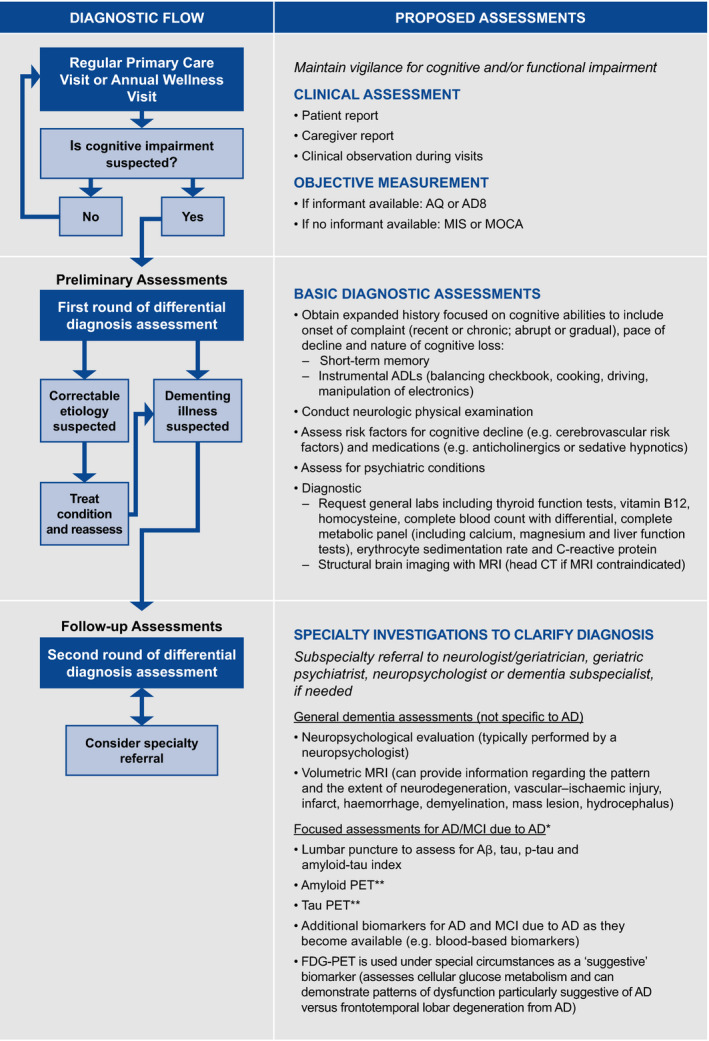
The critical role of primary care clinicians (PCCs) in Alzheimer's disease (AD) prevention, diagnosis and management must evolve as new treatment paradigms and disease-modifying therapies (DMTs) emerge. Our understanding of AD has grown substantially: no longer conceptualized as a late-in-life syndrome of cognitive and functional impairments, we now recognize that AD pathology builds silently for decades before cognitive impairment is detectable. Clinically, AD first manifests subtly as mild cognitive impairment (MCI) due to AD before progressing to dementia. Emerging optimism for improved outcomes in AD stems from a focus on preventive interventions in midlife and timely, biomarker-confirmed diagnosis at early signs of cognitive deficits (i.e. MCI due to AD and mild AD dementia). A timely AD diagnosis is particularly important for optimizing patient care and enabling the appropriate use of anticipated DMTs. An accelerating challenge for PCCs and AD specialists will be to respond to innovations in diagnostics and therapy for AD in a system that is not currently well positioned to do so. To overcome these challenges, PCCs and AD specialists must collaborate closely to navigate and optimize dynamically evolving AD care in the face of new opportunities. In the spirit of this collaboration, we summarize here some prominent and influential models that inform our current understanding of AD. We also advocate for timely and accurate (i.e. biomarker-defined) diagnosis of early AD. In doing so, we consider evolving issues related to prevention, detecting emerging cognitive impairment and the role of biomarkers in the clinic.
Keywords: Alzheimer disease; biomarkers; dementia; disease-modifying therapies; mild cognitive impairment; primary health care.
© 2021 The Authors. Journal of Internal Medicine published by John Wiley & Sons Ltd on behalf of Association for Publication of The Journal of Internal Medicine.
Conflict of interest statement
Dr. Liss reports personal consultancy and educational presentation fees from Acadia, Genentech/Roche, Eisai and Biogen. Dr. Seleri is a full‐time employee of Genentech and receives salary and bonuses, and owns company stock. Dr. Cummings reports grants from NIH/NIGMS and personal fees from Keep Memory Alive. Dr. Cummings reports personal consulting fees from Acadia, Actinogen, AgeneBio, Alkahest, Alzheon, Annovis, Avanir, Axsome, Biogen, BioXcel, Cassava, Cerecin, Cerevel, Cognoptix, Cortexyme, EIP Pharma, Eisai, Foresight, GemVax, Green Valley, Grifols, Hisun, Idorsia, Karuna, Nutricia, Orion, Otsuka, Probiodrug, reMYND, Resverlogix, Roche, Samumed, Samus Therapeutics, Third Rock, Signant Health, Sunovion, Suven, United Neuroscience pharmaceutical and assessment companies, and Alzheimer Drug Discovery Foundation. Dr. Cummings reports stock ownership in ADAMAS, BioAsis, MedAvante, QR Pharma and United Neuroscience, outside the submitted work. In addition, Dr. Cummings has a patent Neuropsychiatric Inventory (NPI) with royalties paid, and Dr. Cummings is the Chief Scientific Advisor for CNS Innovations and a Board member of Keep Memory Alive. Dr. Atri reports receiving grants and personal fees from AbbVie, Biogen, Eisai and Lundbeck. He also reports receiving personal fees from Acadia, Grifols, the Japanese Organization for Medical Device Development, Medical Care Corporation, Novo Nordisk, Roche/Genentech, Suven and Synexus. He also reports receiving grants to his institution for clinical trials and research from Alzheimer’s Clinical Trials Consortium, Alzheimer's Disease Cooperative Study, Alzheimer's Therapeutics Research Institute, American College of Radiology, Arizona Alzheimer’s Research Consortium, Alzheimer's Prevention Initiative, Biohaven, Global Alzheimer’s Platform, Johns Hopkins, Lilly, NIH/NIA, University of Indiana, University of Southern California and vTV. Dr. Atri receives personal fees and book royalties from Oxford University Press, and travel/lodging reimbursement from Alzheimer's Association and NIH/NINDS. Dr. Geldmacher reports grants from Biogen, Eisai, Genentech and Neurium paid directly to institution, and personal fees from Premier Applied Science, Genentech and Grifols. Dr. Candela is an employee of Health & Wellness Partners, LLC, which receives payment from Genentech for services rendered. Dr. Devanand is a scientific adviser for Acadia, Genentech, Sunovion and Eisai; Dr. Devanand is on the Data and Safety Monitoring Board of Green Valley. Dr. Fillit reports receiving personal consulting fees from Alector, Biogen, Samus Therapeutics, vTv, Otsuka and Eli Lilly. Dr. Mintzer reports personal consulting fees from Acadia, Avanir, Biogen, Cerevel and Praxis. Dr. Bittner is an employee of F. Hoffmann‐La Roche AG and owns stock. In addition, Dr. Bittner has a patent around blood‐based biomarkers in AD pending. Dr. Brunton reports serving on advisory boards and speakers bureaus for Acadia. Dr. Kerwin, Dr. Susman, Dr. Clevenger and Dr. Cotter have nothing to disclose. Dr. Jackson reports personal consulting fees from AbbVie, Genentech, Otsuka and Sunovion. Dr. Small reports personal advisor fees from AARP, Acadia, Activis, Genentech, Gerontological Society of America, HANDOK, Lundbeck, Roche, Theravalues and RB Health. In addition, Dr. Small is a co‐inventor of FDDNP‐PET and co‐founder of Ceremark Pharma, LLC. Dr. Grossberg reports personal consulting fees from Acadia, Alkahest, Allergan, Avanir, Biogen, BioXcel, Genentech, Karuna, Lundbeck, Novartis, Otsuka, Roche and Takeda. Dr. Grossberg has received research support from NIA. In addition, Dr. Grossberg serves on Safety Monitoring Committees for EryDel, Newron and Anavex, and on the Data Monitoring Committee for ITI Therapeutics. Dr. Stefanacci reports being an employee of EVERSANA, which provides consulting services to pharmaceutical companies involved in this treatment area (e.g. Biogen). Dr. Wise‐Brown is a full‐time employee of Genentech and receives salary and bonuses, and owns company stock. Dr. Sabbagh reports personal consulting fees from Alzheon, Athira, Biogen, Cortexyme, Danone, Eisai, Neurotrope, Roche–Genentech, Stage 2 Innovations and vTV Therapeutics. Dr. Sabbagh reports ownership interest in Brain Health Inc, NeuroReserve, NeuroTau, Neurotrope, Optimal Cognitive Health Co., Versanum Inc and uMethod Health.
Figures
Comment in
-
Alzheimer's disease in primary care: new tools for improved and simplified diagnostics.J Intern Med. 2021 Aug;290(2):477-479. doi: 10.1111/joim.13249. Epub 2021 Feb 6. J Intern Med. 2021. PMID: 33547829 No abstract available.
References
-
- Alzheimer’s Association Facts and figures. Alzheimers Dement 2020;2020:391–460.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
