

Role of gut microbiota in regulating gastrointestinal dysfunction and motor symptoms in a mouse model of Parkinson's disease
- PMID: 33459114
- PMCID: PMC7833732
- DOI: 10.1080/19490976.2020.1866974
Role of gut microbiota in regulating gastrointestinal dysfunction and motor symptoms in a mouse model of Parkinson's disease
Abstract
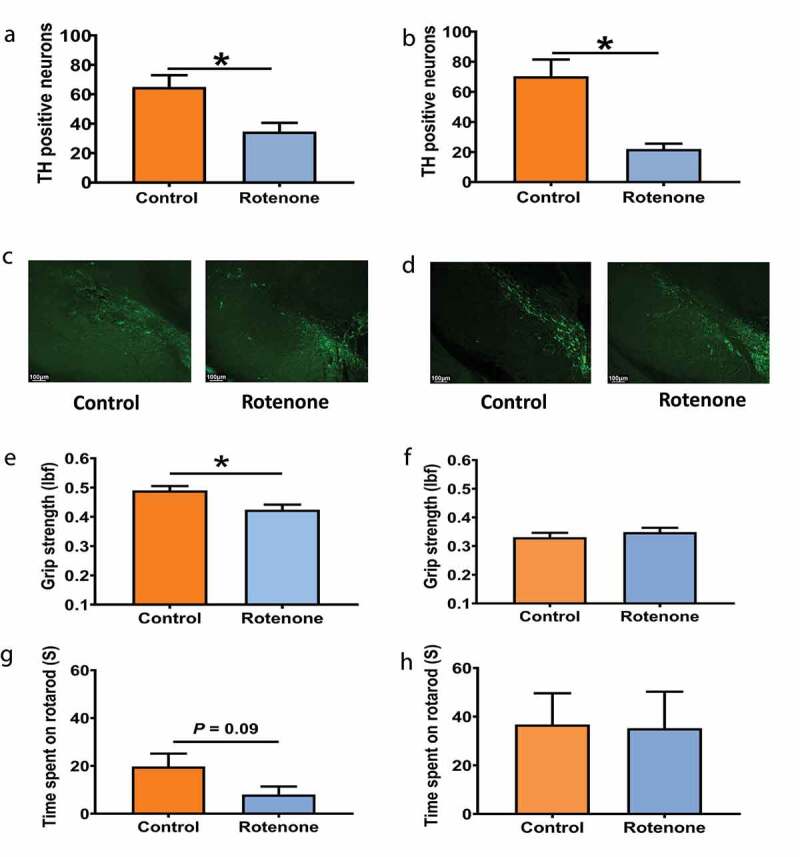
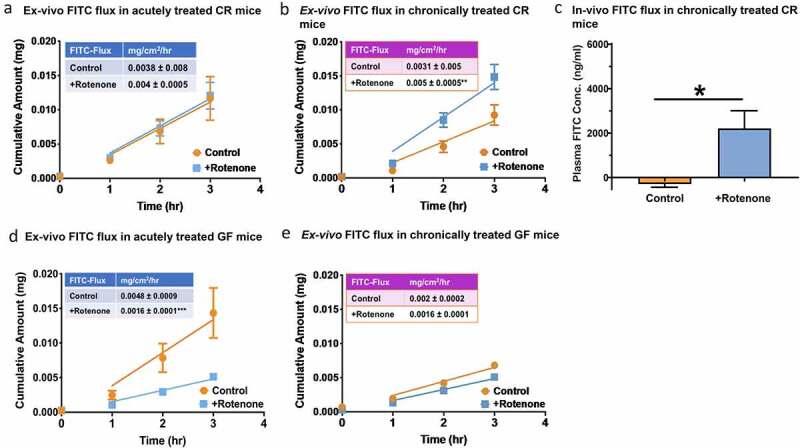
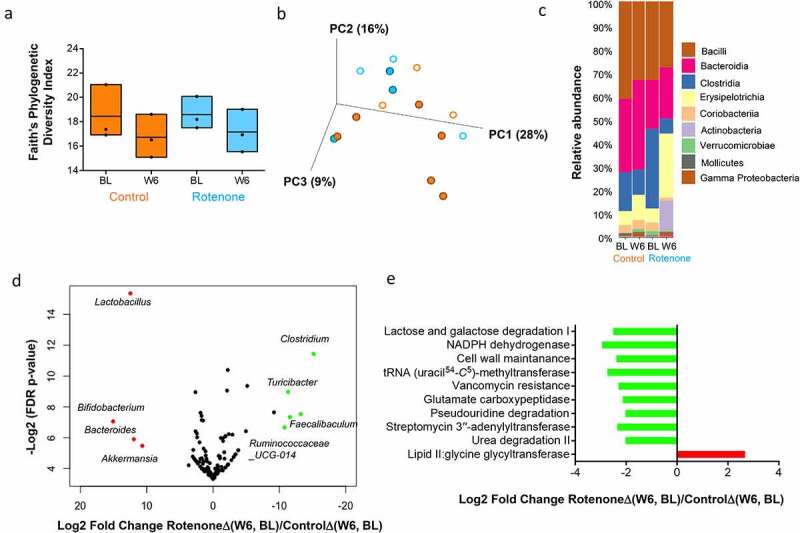
Parkinson's disease (PD) is a common neurodegenerative disorder characterized primarily by motor and non-motor gastrointestinal (GI) deficits. GI symptoms' including compromised intestinal barrier function often accompanies altered gut microbiota composition and motor deficits in PD. Therefore, in this study, we set to investigate the role of gut microbiota and epithelial barrier dysfunction on motor symptom generation using a rotenone-induced mouse model of PD. We found that while six weeks of 10 mg/kg of chronic rotenone administration by oral gavage resulted in loss of tyrosine hydroxylase (TH) neurons in both germ-free (GF) and conventionally raised (CR) mice, the decrease in motor strength and coordination was observed only in CR mice. Chronic rotenone treatment did not disrupt intestinal permeability in GF mice but resulted in a significant change in gut microbiota composition and an increase in intestinal permeability in CR mice. These results highlight the potential role of gut microbiota in regulating barrier dysfunction and motor deficits in PD.
Keywords: Microbiota-gut-brain axis, intestinal epithelial barrier, idiopathic Parkinson's disease, gnotobiotic mice, Braak hypothesis.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical