

Adoptive Transfer of JC Virus-Specific T Lymphocytes for the Treatment of Progressive Multifocal Leukoencephalopathy
- PMID: 33459417
- PMCID: PMC8248385
- DOI: 10.1002/ana.26020
Adoptive Transfer of JC Virus-Specific T Lymphocytes for the Treatment of Progressive Multifocal Leukoencephalopathy
Abstract
Objective: Progressive multifocal leukoencephalopathy (PML) is still burdened by high mortality in a subset of patients, such as those affected by hematological malignancies. The aim of this study was to analyze the safety and carry out preliminary evaluation of the efficacy of polyomavirus JC (JCPyV)-specific T cell therapy in a cohort of hematological patients with PML.
Methods: Between 2014 and 2019, 9 patients with a diagnosis of "definite PML" according to the 2013 consensus who were showing progressive clinical deterioration received JCPyV-specific T cells. Cell lines were expanded from autologous or allogenic peripheral blood mononuclear cells by stimulation with JCPyV antigen-derived peptides.
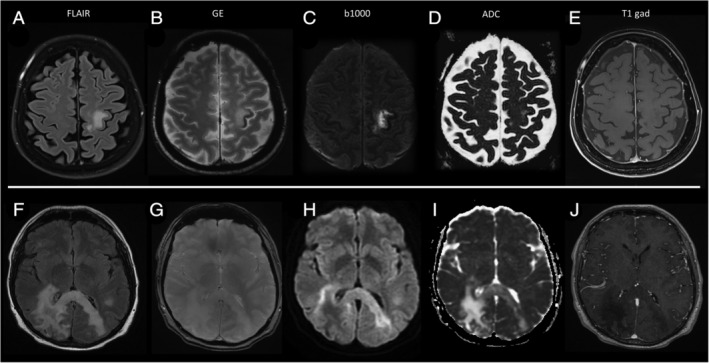
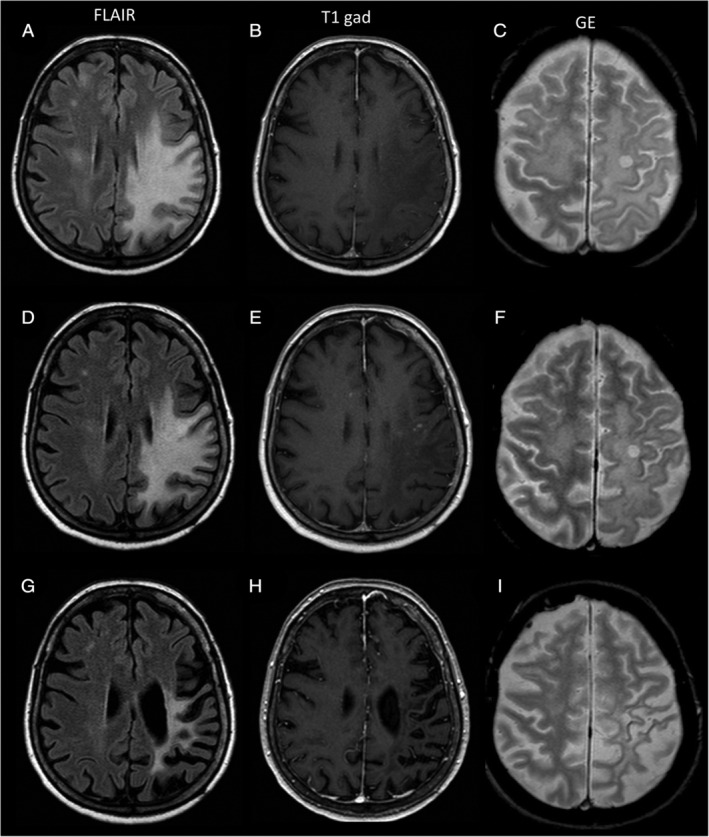
Results: None of the patients experienced treatment-related adverse events. In the evaluable patients, an increase in the frequency of circulating JCPyV-specific lymphocytes was observed, with a decrease or clearance of JCPyV viral load in cerebrospinal fluid. In responsive patients, transient appearance of punctate areas of contrast enhancement within, or close to, PML lesions was observed, which was interpreted as a sign of immune control and which regressed spontaneously without the need for steroid treatment. Six of 9 patients achieved PML control, with 5 alive and in good clinical condition at their last follow-up.
Interpretation: Among other novel treatments, T cell therapy is emerging as a viable treatment option in patients with PML, particularly for those not amenable to restoration of specific immunity. Neurologists should be encouraged to refer PML patients to specialized centers to allow access to this treatment strategy. ANN NEUROL 2021;89:769-779.
© 2021 The Authors. Annals of Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
Nothing to report.
Figures
Similar articles
-
BK virus-specific T cells for immunotherapy of progressive multifocal leukoencephalopathy: an open-label, single-cohort pilot study.Lancet Neurol. 2021 Aug;20(8):639-652. doi: 10.1016/S1474-4422(21)00174-5. Lancet Neurol. 2021. PMID: 34302788 Free PMC article.
-
Adoptive JC Virus-Specific T Lymphocytes for the Treatment of Progressive Multifocal Leukoencephalopathy: Experience from Two Italian Centers.Viruses. 2025 Jun 30;17(7):934. doi: 10.3390/v17070934. Viruses. 2025. PMID: 40733551 Free PMC article.
-
High expression of JC polyomavirus-encoded microRNAs in progressive multifocal leukoencephalopathy tissues and its repressive role in virus replication.PLoS Pathog. 2020 Apr 23;16(4):e1008523. doi: 10.1371/journal.ppat.1008523. eCollection 2020 Apr. PLoS Pathog. 2020. PMID: 32324824 Free PMC article.
-
Advances in Treatment of Progressive Multifocal Leukoencephalopathy.Ann Neurol. 2021 Dec;90(6):865-873. doi: 10.1002/ana.26198. Epub 2021 Sep 7. Ann Neurol. 2021. PMID: 34405435 Free PMC article. Review.
-
Progressive multifocal leukoencephalopathy and the spectrum of JC virus-related disease.Nat Rev Neurol. 2021 Jan;17(1):37-51. doi: 10.1038/s41582-020-00427-y. Epub 2020 Nov 20. Nat Rev Neurol. 2021. PMID: 33219338 Free PMC article. Review.
Cited by
-
JC Virus in Kidney Transplant Population: Are We Cautious Enough?J Clin Med. 2024 Apr 11;13(8):2217. doi: 10.3390/jcm13082217. J Clin Med. 2024. PMID: 38673491 Free PMC article. Review.
-
Progressive multifocal leukoencephalopathy following obinutuzumab and bendamustine therapy for follicular lymphoma: case report and literature review.Acta Neurol Belg. 2024 Dec;124(6):2085-2089. doi: 10.1007/s13760-024-02580-3. Epub 2024 May 27. Acta Neurol Belg. 2024. PMID: 38801626 No abstract available.
-
Viral meningoencephalitis in pediatric solid organ or hematopoietic cell transplant recipients: a diagnostic and therapeutic approach.Front Pediatr. 2024 Feb 12;12:1259088. doi: 10.3389/fped.2024.1259088. eCollection 2024. Front Pediatr. 2024. PMID: 38410764 Free PMC article. Review.
-
Therapeutic advances in neuroinfectious diseases.Ther Adv Infect Dis. 2024 Sep 20;11:20499361241274246. doi: 10.1177/20499361241274246. eCollection 2024 Jan-Dec. Ther Adv Infect Dis. 2024. PMID: 39314743 Free PMC article. Review.
-
BK virus-specific T cells for immunotherapy of progressive multifocal leukoencephalopathy: an open-label, single-cohort pilot study.Lancet Neurol. 2021 Aug;20(8):639-652. doi: 10.1016/S1474-4422(21)00174-5. Lancet Neurol. 2021. PMID: 34302788 Free PMC article.
References
-
- Pavlovic D, Patel MA, Patera AC, et al. T cell deficiencies as a common risk factor for drug associated progressive multifocal leukoencephalopathy. Immunobiology 2018;223:508–517. - PubMed
-
- Engsig FN, Hansen A‐BE, Omland LH, et al. Incidence, clinical presentation, and outcome of progressive multifocal leukoencephalopathy in HIV‐infected patients during the highly active antiretroviral therapy era: a nationwide cohort study. J Infect Dis 2009;199:77–83. - PubMed
-
- García‐Suárez J, de Miguel D, Krsnik I, et al. Changes in the natural history of progressive multifocal leukoencephalopathy in HIV‐negative lymphoproliferative disorders: impact of novel therapies. Am J Hematol 2005;80:271–281. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
