

Diagnosis and treatment of cardiac amyloidosis: position statement of the German Cardiac Society (DGK)
- PMID: 33459839
- PMCID: PMC8055575
- DOI: 10.1007/s00392-020-01799-3
Diagnosis and treatment of cardiac amyloidosis: position statement of the German Cardiac Society (DGK)
Abstract
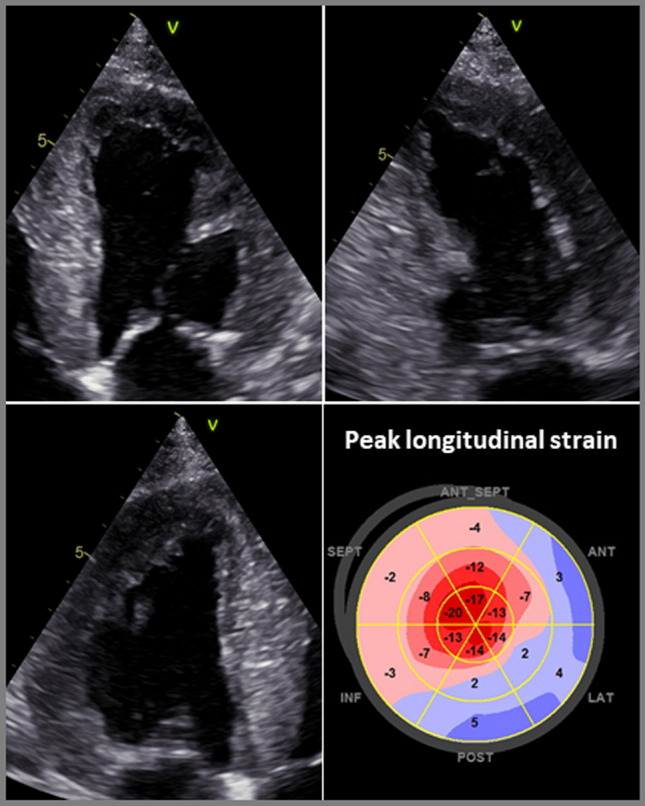
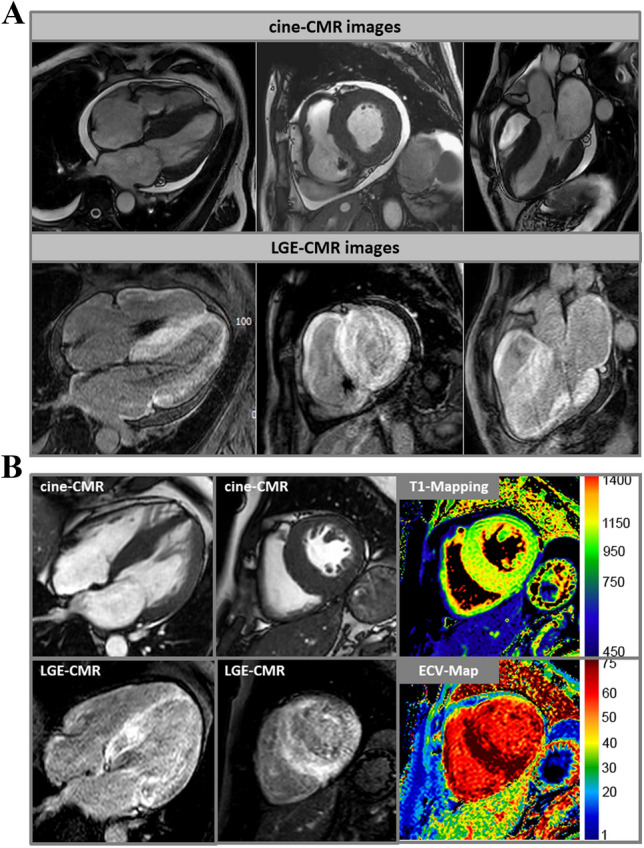
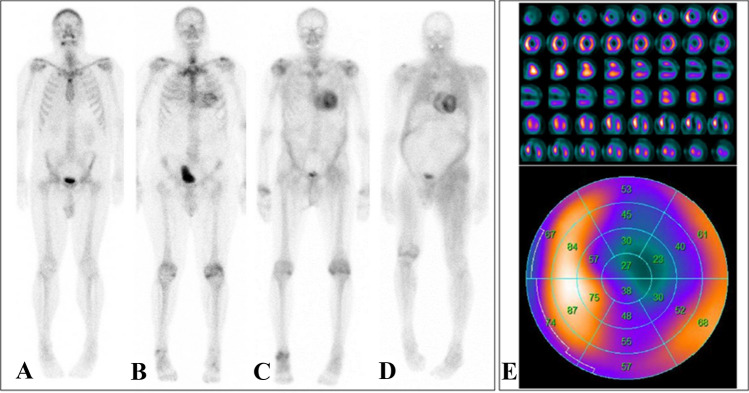
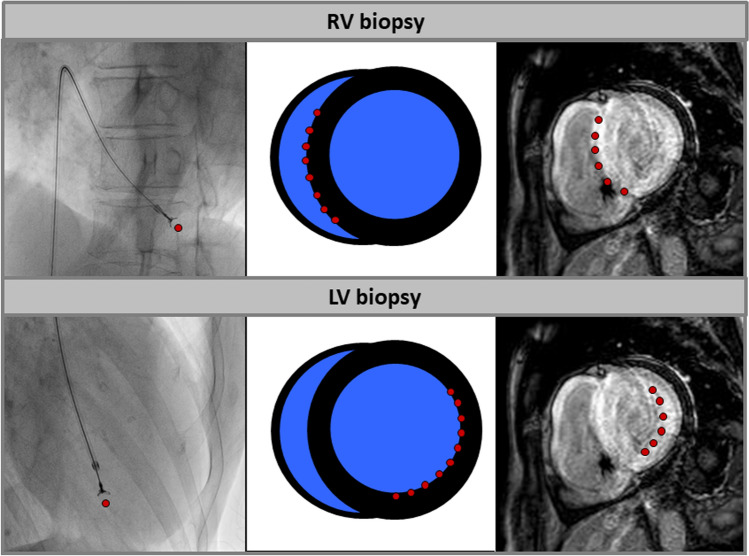
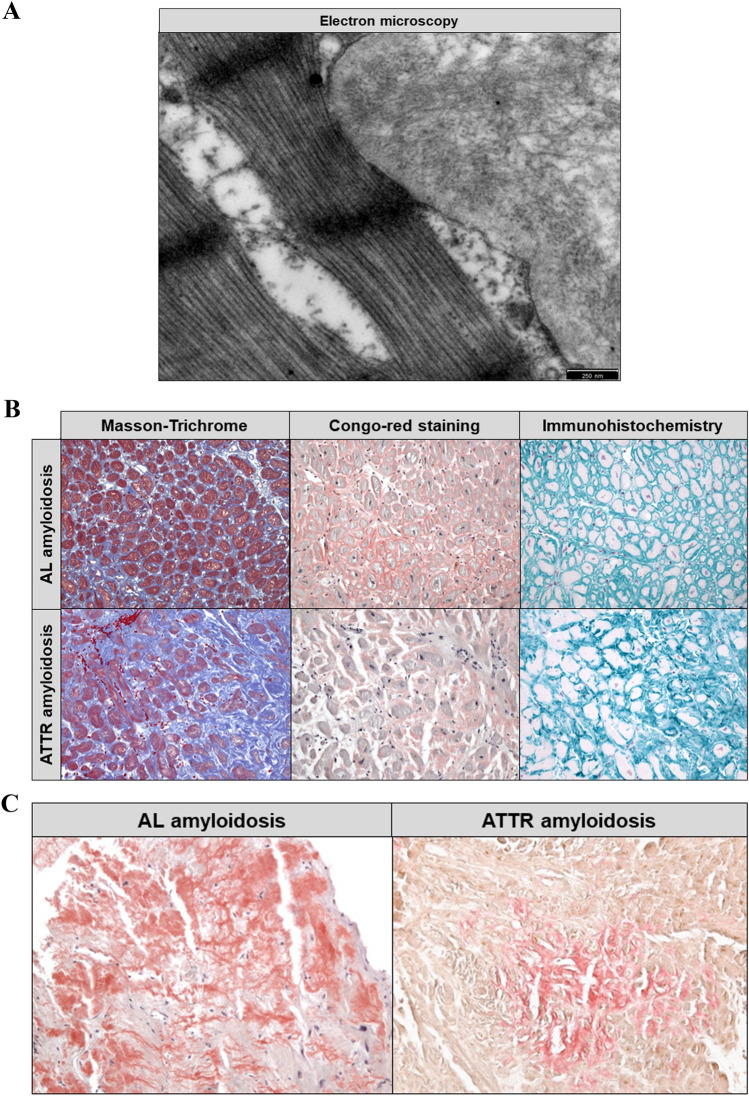
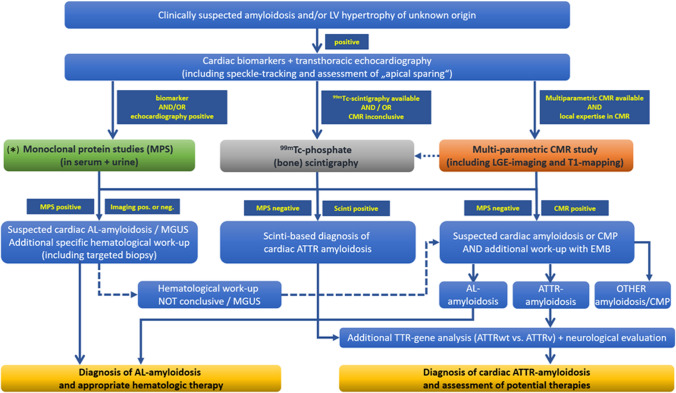
Systemic forms of amyloidosis affecting the heart are mostly light-chain (AL) and transthyretin (ATTR) amyloidoses. The latter is caused by deposition of misfolded transthyretin, either in wild-type (ATTRwt) or mutant (ATTRv) conformation. For diagnostics, specific serum biomarkers and modern non-invasive imaging techniques, such as cardiovascular magnetic resonance imaging (CMR) and scintigraphic methods, are available today. These imaging techniques do not only complement conventional echocardiography, but also allow for accurate assessment of the extent of cardiac involvement, in addition to diagnosing cardiac amyloidosis. Endomyocardial biopsy still plays a major role in the histopathological diagnosis and subtyping of cardiac amyloidosis. The main objective of the diagnostic algorithm outlined in this position statement is to detect cardiac amyloidosis as reliably and early as possible, to accurately determine its extent, and to reliably identify the underlying subtype of amyloidosis, thereby enabling subsequent targeted treatment.
Keywords: Amyloidosis; Endomyocardial biopsy; Magnetic resonance imaging; Myocardium; Scintigraphy.
Conflict of interest statement
Ali Yilmaz: speaker and consultant activities for Alnylam, Pfizer Pharma GmbH and Akcea Therapeutics; research cooperation with Philips. Johann Bauersachs: speaker and consultant activities for Pfizer Pharma GmbH. Frank Bengel: speaker and consultant activities for Siemens Healthineers, GE Healthcare, Alnylam and Pfizer Pharma GmbH. Ronny Büchel: speaker honoraria from Pfizer Pharma GmbH and GE Healthcare. Ingrid Kindermann: speaker honoraria from Akcea Therapeutics, Alnylam and Pfizer Pharma GmbH. Karin Klingel: speaker honoraria from Akcea Therapeutics, Alnylam and Pfizer Pharma GmbH. Fabian Knebel: speaker and consultant activities for Akcea Therapeutics, Alnylam and Pfizer Pharma GmbH. Benjamin Meder and Fabian aus dem Siepen: speaker honoraria from Akcea Therapeutics, Pfizer Pharma GmbH and Alnylam as well as travel grants from Pfizer Pharma GmbH. Caroline Morbach: research cooperation with the University of Würzburg and Tomtec Imaging Systems funded by a research grant from the Bavarian Ministry of Economic Affairs, Regional Development and Energy, Germany; speakers honorarium and travel grants from Amgen, Tomtec, Orion Pharma, and Alnylam; participation in Advisory and Patient Eligibility Boards sponsored by Akcea, Alnylam, Pfizer, and EBR Systems; principal investigator in trials sponsored by Alnylam and AstraZeneca. Eike Nagel: speaker honoraria from Bayer AG and Neosoft; research cooperation with Bayer AG. Eric Schulze-Bahr: None. Norbert Frey: None.
Figures
References
-
- Vaxman I, Gertz M. Recent advances in the diagnosis, risk stratification, and management of systemic light-chain amyloidosis. Acta Haematol. 2019;141(2):93–106. - PubMed
-
- Ihne S, Morbach C, Obici L, Palladini G, Störk S. Amyloidosis in heart failure. Curr Heart Fail Rep. 2019;16(6):285–303. - PubMed
-
- Palladini G, Russo P, Bosoni T, Verga L, Sarais G, Lavatelli F, Nuvolone M, Obici L, Casarini S, Donadei S, Albertini R, Righetti G, Marini M, Graziani MS, Melzi D’Eril GV, Moratti R, Merlini G. Identification of amyloidogenic light chains requires the combination of serum-free light chain assay with immunofixation of serum and urine. Clin Chem. 2009;55(3):499–504. doi: 10.1373/clinchem.2008.117143. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
