

Characteristics, Outcomes, and Trends of Patients With COVID-19-Related Critical Illness at a Learning Health System in the United States
- PMID: 33460330
- PMCID: PMC7901669
- DOI: 10.7326/M20-5327
Characteristics, Outcomes, and Trends of Patients With COVID-19-Related Critical Illness at a Learning Health System in the United States
Abstract
Background: The coronavirus disease 2019 (COVID-19) pandemic continues to surge in the United States and globally.
Objective: To describe the epidemiology of COVID-19-related critical illness, including trends in outcomes and care delivery.
Design: Single-health system, multihospital retrospective cohort study.
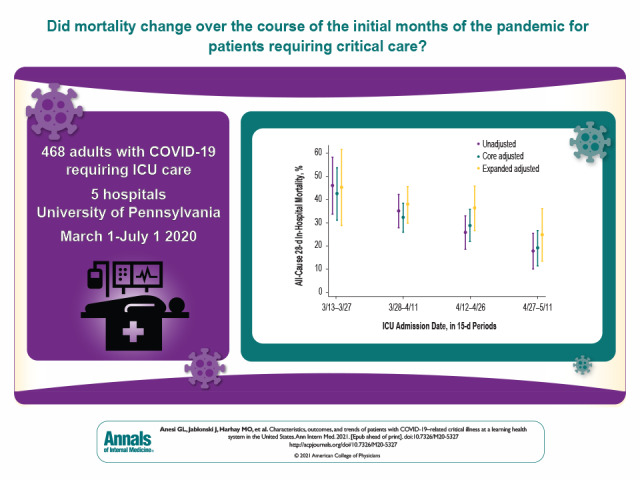
Setting: 5 hospitals within the University of Pennsylvania Health System.
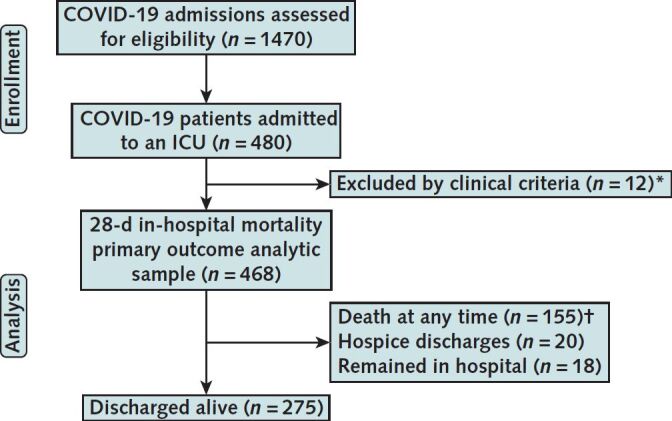
Patients: Adults with COVID-19-related critical illness who were admitted to an intensive care unit (ICU) with acute respiratory failure or shock during the initial surge of the pandemic.
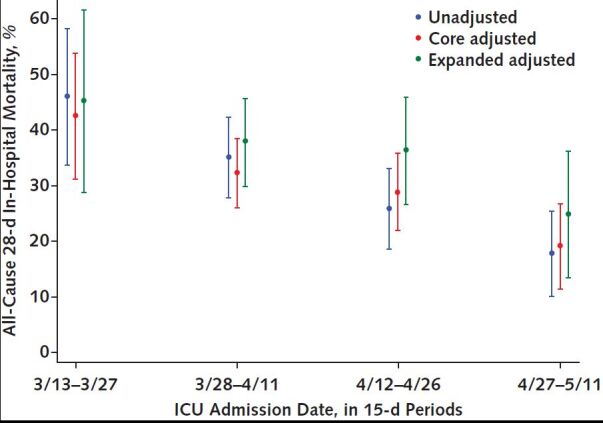
Measurements: The primary exposure for outcomes and care delivery trend analyses was longitudinal time during the pandemic. The primary outcome was all-cause 28-day in-hospital mortality. Secondary outcomes were all-cause death at any time, receipt of mechanical ventilation (MV), and readmissions.
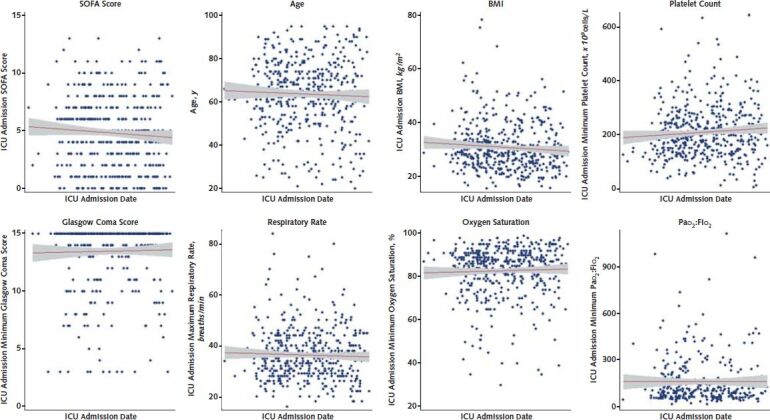
Results: Among 468 patients with COVID-19-related critical illness, 319 (68.2%) were treated with MV and 121 (25.9%) with vasopressors. Outcomes were notable for an all-cause 28-day in-hospital mortality rate of 29.9%, a median ICU stay of 8 days (interquartile range [IQR], 3 to 17 days), a median hospital stay of 13 days (IQR, 7 to 25 days), and an all-cause 30-day readmission rate (among nonhospice survivors) of 10.8%. Mortality decreased over time, from 43.5% (95% CI, 31.3% to 53.8%) to 19.2% (CI, 11.6% to 26.7%) between the first and last 15-day periods in the core adjusted model, whereas patient acuity and other factors did not change.
Limitations: Single-health system study; use of, or highly dynamic trends in, other clinical interventions were not evaluated, nor were complications.
Conclusion: Among patients with COVID-19-related critical illness admitted to ICUs of a learning health system in the United States, mortality seemed to decrease over time despite stable patient characteristics. Further studies are necessary to confirm this result and to investigate causal mechanisms.
Primary funding source: Agency for Healthcare Research and Quality.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical