

Predictive value of the neutrophil to lymphocyte ratio for disease deterioration and serious adverse outcomes in patients with COVID-19: a prospective cohort study
- PMID: 33461497
- PMCID: PMC7812552
- DOI: 10.1186/s12879-021-05796-3
Predictive value of the neutrophil to lymphocyte ratio for disease deterioration and serious adverse outcomes in patients with COVID-19: a prospective cohort study
Abstract
Background: Early identification of patients who are at high risk of poor clinical outcomes is of great importance in saving the lives of patients with novel coronavirus disease 2019 (COVID-19) in the context of limited medical resources.
Objective: To evaluate the value of the neutrophil to lymphocyte ratio (NLR), calculated at hospital admission and in isolation, for the prediction of the subsequent presence of disease progression and serious clinical outcomes (e.g., shock, death).
Methods: We designed a prospective cohort study of 352 hospitalized patients with COVID-19 between January 9 and February 26, 2020, in Yichang City, Hubei Province. Patients with an NLR equal to or higher than the cutoff value derived from the receiver operating characteristic curve method were classified as the exposed group. The primary outcome was disease deterioration, defined as an increase of the clinical disease severity classification during hospitalization (e.g., moderate to severe/critical; severe to critical). The secondary outcomes were shock and death during the treatment.
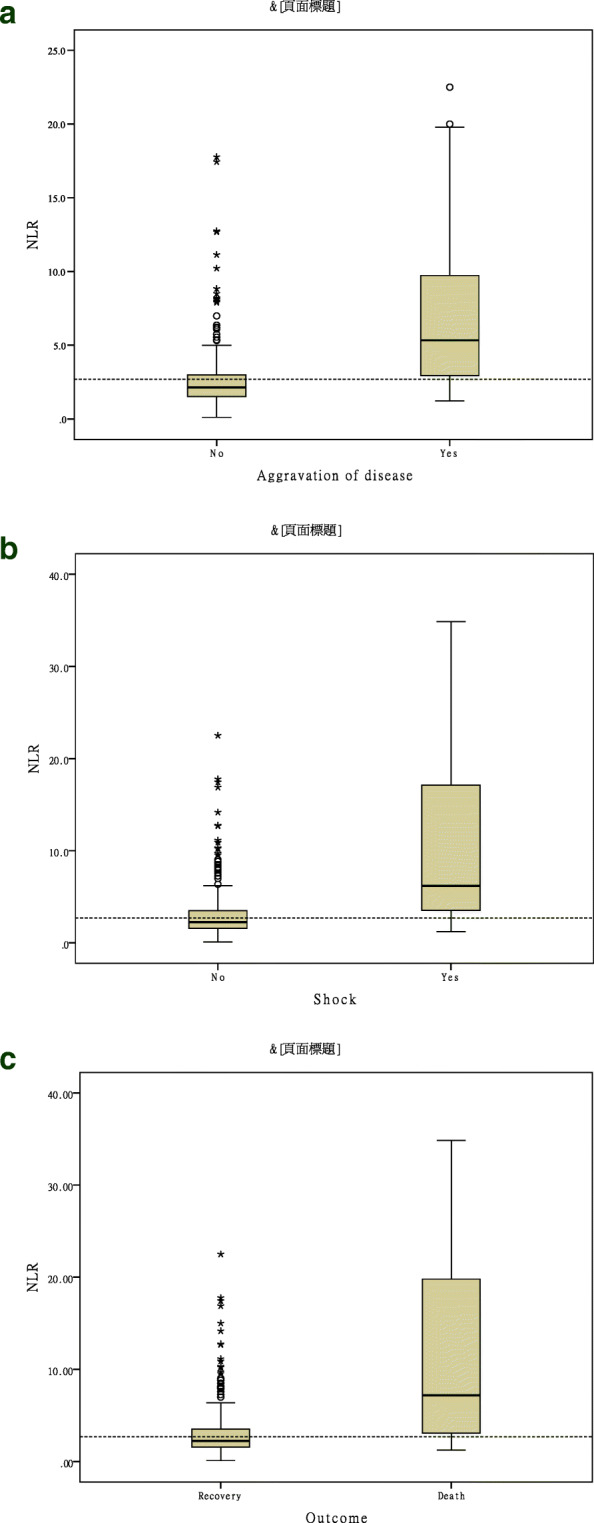
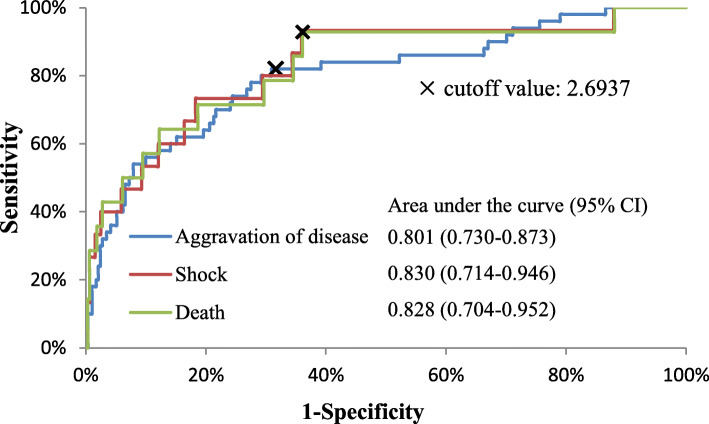
Results: During the follow-up period, 51 (14.5%) patients' conditions deteriorated, 15 patients (4.3%) had complicated septic shock, and 15 patients (4.3%) died. The NLR was higher in patients with deterioration than in those without deterioration (median: 5.33 vs. 2.14, P < 0.001), and higher in patients with serious clinical outcomes than in those without serious clinical outcomes (shock vs. no shock: 6.19 vs. 2.25, P < 0.001; death vs. survival: 7.19 vs. 2.25, P < 0.001). The NLR measured at hospital admission had high value in predicting subsequent disease deterioration, shock and death (all the areas under the curve > 0.80). The sensitivity of an NLR ≥ 2.6937 for predicting subsequent disease deterioration, shock and death was 82.0% (95% confidence interval, 69.0 to 91.0), 93.3% (68.0 to 100), and 92.9% (66.0 to 100), and the corresponding negative predictive values were 95.7% (93.0 to 99.2), 99.5% (98.6 to 100) and 99.5% (98.6 to 100), respectively.
Conclusions: The NLR measured at admission and in isolation can be used to effectively predict the subsequent presence of disease deterioration and serious clinical outcomes in patients with COVID-19.
Keywords: COVID-19; Death; Deterioration; Neutrophil to lymphocyte ratio; Shock.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Neutrophil-to-lymphocyte ratio as a prognostic indicator in COVID-19: Evidence from a northern tanzanian cohort.PLoS One. 2025 Jan 31;20(1):e0300231. doi: 10.1371/journal.pone.0300231. eCollection 2025. PLoS One. 2025. PMID: 39888959 Free PMC article.
-
[Value of neutrophil-to-lymphocyte ratio in the classification diagnosis of coronavirus disease 2019].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020 May;32(5):554-558. doi: 10.3760/cma.j.cn121430-20200413-00506. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020. PMID: 32576346 Chinese.
-
The use of neutrophil-to-lymphocyte ratio (NLR) as a marker for COVID-19 infection in Saudi Arabia: A case-control retrospective multicenter study.Saudi Med J. 2021 Apr;42(4):370-376. doi: 10.15537/smj.2021.42.4.20200818. Saudi Med J. 2021. PMID: 33795491 Free PMC article.
-
Neutrophil-to-lymphocyte ratio on admission to predict the severity and mortality of COVID-19 patients: A meta-analysis.Am J Emerg Med. 2021 Apr;42:60-69. doi: 10.1016/j.ajem.2021.01.006. Epub 2021 Jan 9. Am J Emerg Med. 2021. PMID: 33453617 Free PMC article.
-
The Impact of Neutrophil-Lymphocyte Count Ratio in COVID-19: A Systematic Review and Meta-Analysis.J Intensive Care Med. 2022 Jul;37(7):857-869. doi: 10.1177/08850666211045626. Epub 2021 Oct 21. J Intensive Care Med. 2022. PMID: 34672824 Free PMC article.
Cited by
-
Neutrophil-to-Lymphocyte Ratio as a Predictor of Disease Severity and Mortality in Coronavirus Disease 2019: Prospective Study From Central India.Cureus. 2022 Mar 31;14(3):e23696. doi: 10.7759/cureus.23696. eCollection 2022 Mar. Cureus. 2022. PMID: 35519791 Free PMC article.
-
The Role of Hemogram-derived Ratios in COVID-19 Severity Stratification in a Primary Healthcare Facility.Acta Inform Med. 2023 Mar;31(1):41-47. doi: 10.5455/aim.2023.31.41-47. Acta Inform Med. 2023. PMID: 37038490 Free PMC article.
-
The Predictive Role of NLR, d-NLR, MLR, and SIRI in COVID-19 Mortality.Diagnostics (Basel). 2022 Jan 6;12(1):122. doi: 10.3390/diagnostics12010122. Diagnostics (Basel). 2022. PMID: 35054289 Free PMC article.
-
Identifying COVID-19 Confirmed Patients at Elevated Risk for Mortality and Need of Mechanical Ventilation Using a Novel Criteria for Hyperinflammatory Syndrome: A Retrospective Cohort, Single-center, Validation Study.Acta Med Philipp. 2025 Feb 28;59(3):104-115. doi: 10.47895/amp.vi0.9370. eCollection 2025. Acta Med Philipp. 2025. PMID: 40151221 Free PMC article.
-
Plasma-induced nanoparticle aggregation for stratifying COVID-19 patients according to disease severity.Sens Actuators B Chem. 2022 Dec 15;373:132638. doi: 10.1016/j.snb.2022.132638. Epub 2022 Sep 15. Sens Actuators B Chem. 2022. PMID: 36124254 Free PMC article.
References
-
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;23(13):1239–42. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
