

Effect of green-Mediterranean diet on intrahepatic fat: the DIRECT PLUS randomised controlled trial
- PMID: 33461965
- PMCID: PMC8515100
- DOI: 10.1136/gutjnl-2020-323106
Effect of green-Mediterranean diet on intrahepatic fat: the DIRECT PLUS randomised controlled trial
Abstract
Objective: To examine the effectiveness of green-Mediterranean (MED) diet, further restricted in red/processed meat, and enriched with green plants and polyphenols on non-alcoholic fatty liver disease (NAFLD), reflected by intrahepatic fat (IHF) loss.
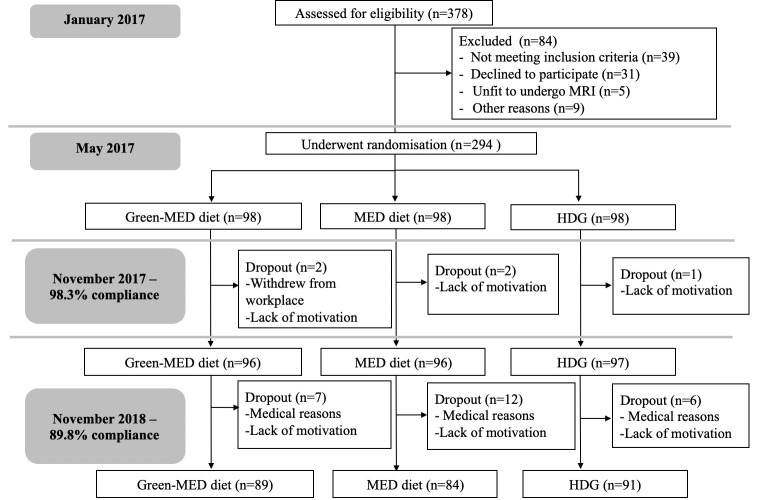
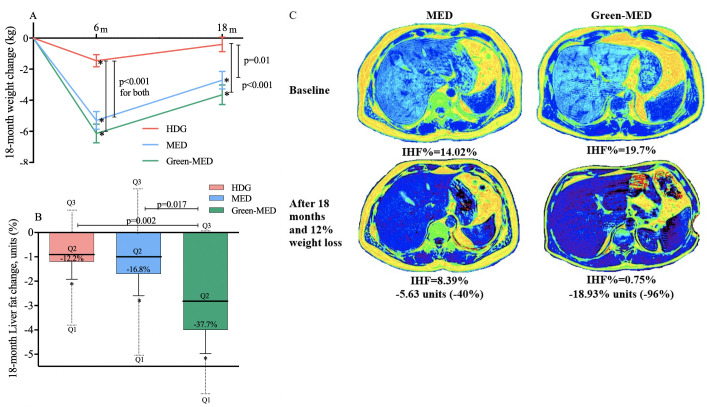
Design: For the DIRECT-PLUS 18-month randomized clinical trial, we assigned 294 participants with abdominal obesity/dyslipidaemia into healthy dietary guidelines (HDG), MED and green-MED weight-loss diet groups, all accompanied by physical activity. Both isocaloric MED groups consumed 28 g/day walnuts (+440 mg/day polyphenols provided). The green-MED group further consumed green tea (3-4 cups/day) and Mankai (a Wolffia globosa aquatic plant strain; 100 g/day frozen cubes) green shake (+1240 mg/day total polyphenols provided). IHF% 18-month changes were quantified continuously by proton magnetic resonance spectroscopy (MRS).
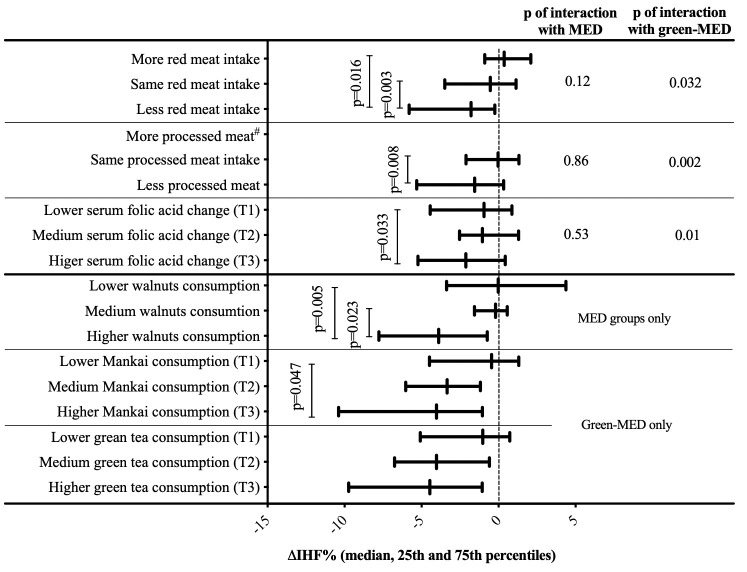
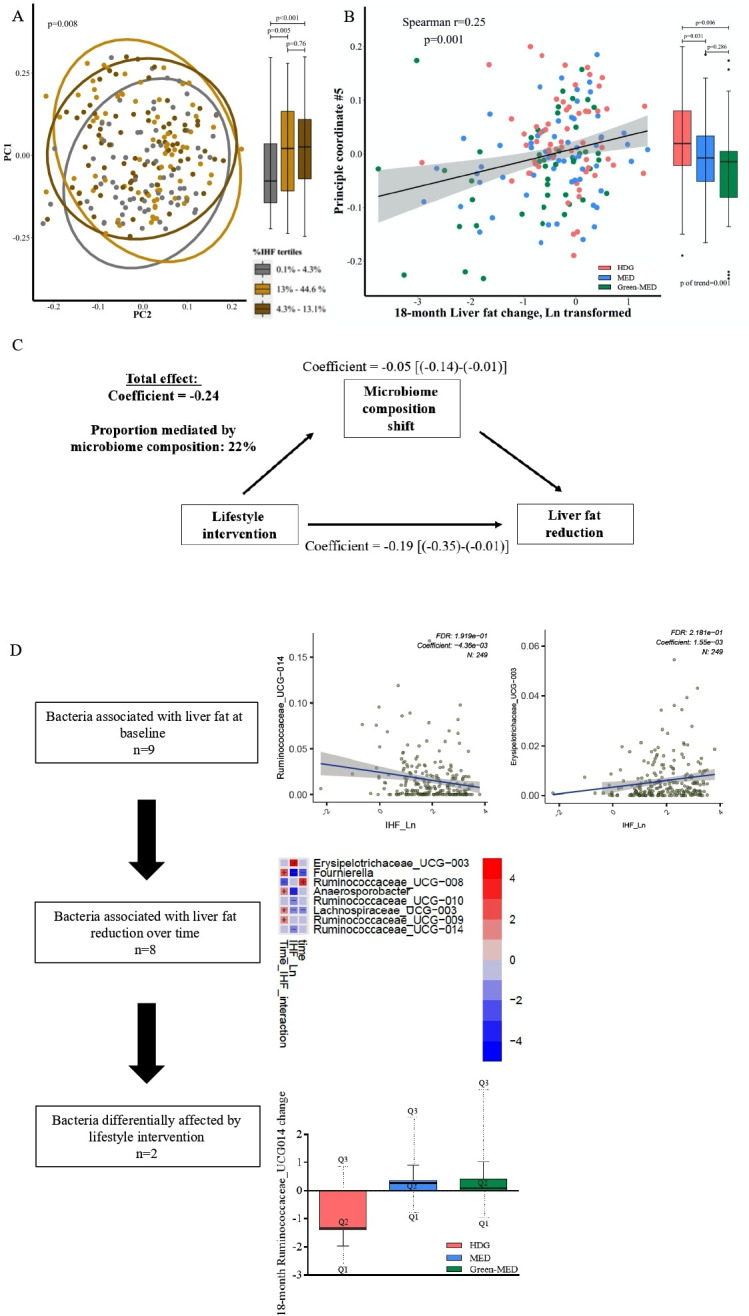
Results: Participants (age=51 years; 88% men; body mass index=31.3 kg/m2; median IHF%=6.6%; mean=10.2%; 62% with NAFLD) had 89.8% 18-month retention-rate, and 78% had eligible follow-up MRS. Overall, NAFLD prevalence declined to: 54.8% (HDG), 47.9% (MED) and 31.5% (green-MED), p=0.012 between groups. Despite similar moderate weight-loss in both MED groups, green-MED group achieved almost double IHF% loss (-38.9% proportionally), as compared with MED (-19.6% proportionally; p=0.035 weight loss adjusted) and HDG (-12.2% proportionally; p<0.001). After 18 months, both MED groups had significantly higher total plasma polyphenol levels versus HDG, with higher detection of Naringenin and 2-5-dihydroxybenzoic-acid in green-MED. Greater IHF% loss was independently associated with increased Mankai and walnuts intake, decreased red/processed meat consumption, improved serum folate and adipokines/lipids biomarkers, changes in microbiome composition (beta-diversity) and specific bacteria (p<0.05 for all).
Conclusion: The new suggested strategy of green-Mediterranean diet, amplified with green plant-based proteins/polyphenols as Mankai, green tea, and walnuts, and restricted in red/processed meat can double IHF loss than other healthy nutritional strategies and reduce NAFLD in half.
Trial registration number: NCT03020186.
Keywords: epidemiology; fatty liver; magnetic resonance imaging; nutrition.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: IS advises to the Hinoman, Ltd. nutritional committee. Youngster is medical advisor for Mybiotix Ltd.
Figures
Comment in
-
Commentary on "Effect of green-Mediterranean diet on intrahepatic fat: the DIRECT PLUS randomised controlled trial".Hepatobiliary Surg Nutr. 2021 Oct;10(5):699-701. doi: 10.21037/hbsn-21-280. Hepatobiliary Surg Nutr. 2021. PMID: 34760978 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical