

CHARGE-AF in a national routine primary care electronic health records database in the Netherlands: validation for 5-year risk of atrial fibrillation and implications for patient selection in atrial fibrillation screening
- PMID: 33462107
- PMCID: PMC7816907
- DOI: 10.1136/openhrt-2020-001459
CHARGE-AF in a national routine primary care electronic health records database in the Netherlands: validation for 5-year risk of atrial fibrillation and implications for patient selection in atrial fibrillation screening
Erratum in
-
Correction: CHARGE-AF in a national routineprimary care electronic health recordsdatabase in the Netherlands: validationfor 5-year risk of atrial fibrillation andimplications for patient selection inatrial fibrillation screening.Open Heart. 2021 Oct;8(2):1. doi: 10.1136/openhrt-2020-001459corr1. Open Heart. 2021. PMID: 34663753 Free PMC article. No abstract available.
Abstract
Aims: To validate a multivariable risk prediction model (Cohorts for Heart and Aging Research in Genomic Epidemiology model for atrial fibrillation (CHARGE-AF)) for 5-year risk of atrial fibrillation (AF) in routinely collected primary care data and to assess CHARGE-AF's potential for automated, low-cost selection of patients at high risk for AF based on routine primary care data.
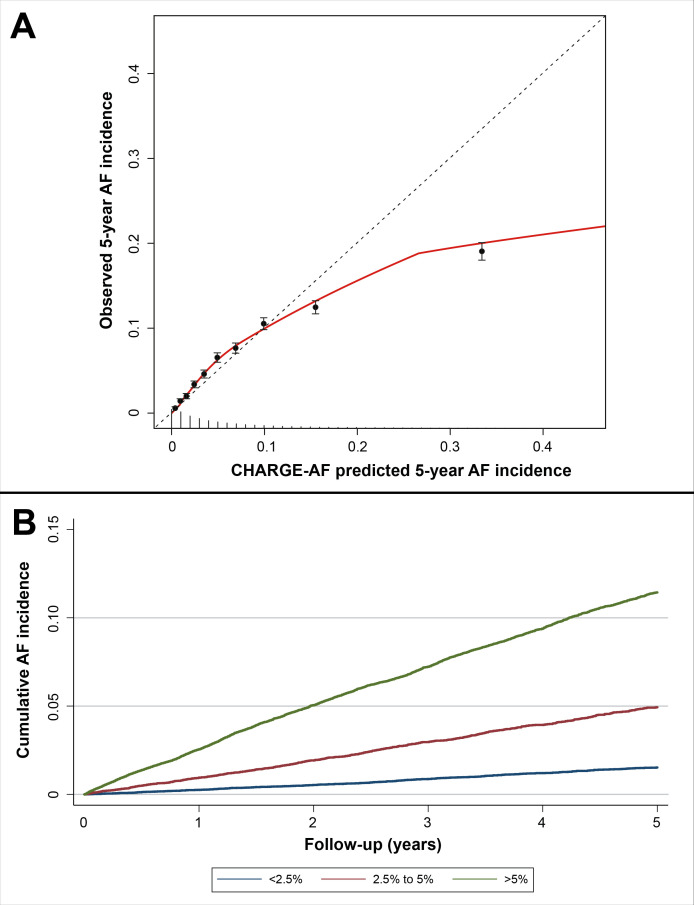
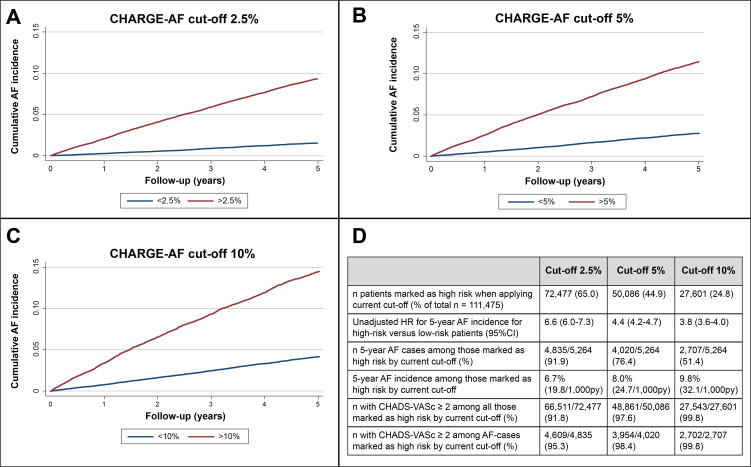
Methods: We included patients aged ≥40 years, free of AF and with complete CHARGE-AF variables at baseline, 1 January 2014, in a representative, nationwide routine primary care database in the Netherlands (Nivel-PCD). We validated CHARGE-AF for 5-year observed AF incidence using the C-statistic for discrimination, and calibration plot and stratified Kaplan-Meier plot for calibration. We compared CHARGE-AF with other predictors and assessed implications of using different CHARGE-AF cut-offs to select high-risk patients.
Results: Among 111 475 patients free of AF and with complete CHARGE-AF variables at baseline (17.2% of all patients aged ≥40 years and free of AF), mean age was 65.5 years, and 53% were female. Complete CHARGE-AF cases were older and had higher AF incidence and cardiovascular comorbidity rate than incomplete cases. There were 5264 (4.7%) new AF cases during 5-year follow-up among complete cases. CHARGE-AF's C-statistic for new AF was 0.74 (95% CI 0.73 to 0.74). The calibration plot showed slight risk underestimation in low-risk deciles and overestimation of absolute AF risk in those with highest predicted risk. The Kaplan-Meier plot with categories <2.5%, 2.5%-5% and >5% predicted 5-year risk was highly accurate. CHARGE-AF outperformed CHA2DS2-VASc (Cardiac failure or dysfunction, Hypertension, Age >=75 [Doubled], Diabetes, Stroke [Doubled]-Vascular disease, Age 65-74, and Sex category [Female]) and age alone as predictors for AF. Dichotomisation at cut-offs of 2.5%, 5% and 10% baseline CHARGE-AF risk all showed merits for patient selection in AF screening efforts.
Conclusion: In patients with complete baseline CHARGE-AF data through routine Dutch primary care, CHARGE-AF accurately assessed AF risk among older primary care patients, outperformed both CHA2DS2-VASc and age alone as predictors for AF and showed potential for automated, low-cost patient selection in AF screening.
Keywords: atrial fibrillation; electronic health records; epidemiology; risk factors.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Magnussen C, Niiranen TJ, Ojeda FM, et al. . Sex differences and similarities in atrial fibrillation epidemiology, risk factors, and mortality in community cohorts: results from the BiomarCaRE Consortium (biomarker for cardiovascular risk assessment in Europe). Circulation 2017;136:1588–97. 10.1161/CIRCULATIONAHA.117.028981 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical