

Modelling the global burden of drug-resistant tuberculosis avertable by a post-exposure vaccine
- PMID: 33462224
- PMCID: PMC7814030
- DOI: 10.1038/s41467-020-20731-x
Modelling the global burden of drug-resistant tuberculosis avertable by a post-exposure vaccine
Abstract
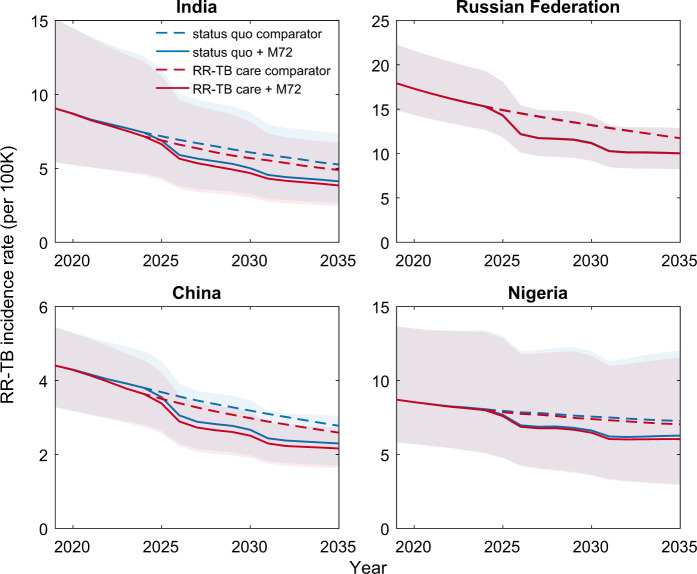
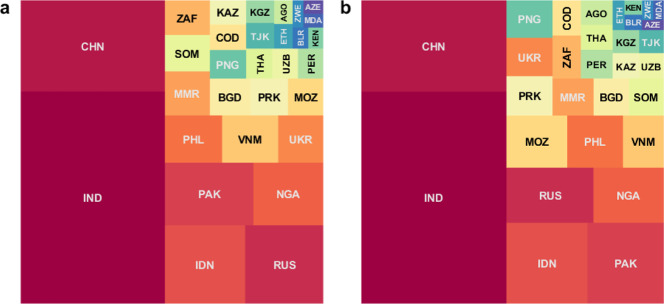
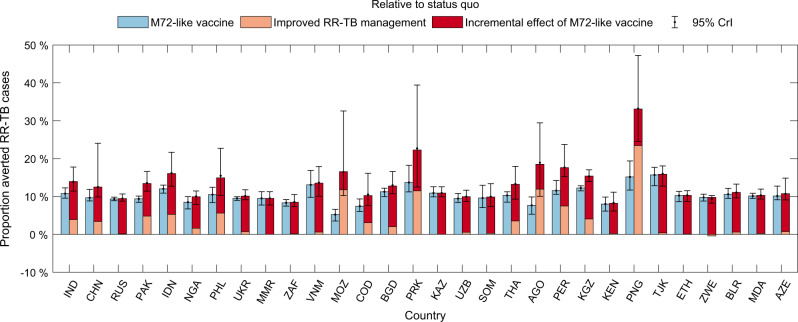
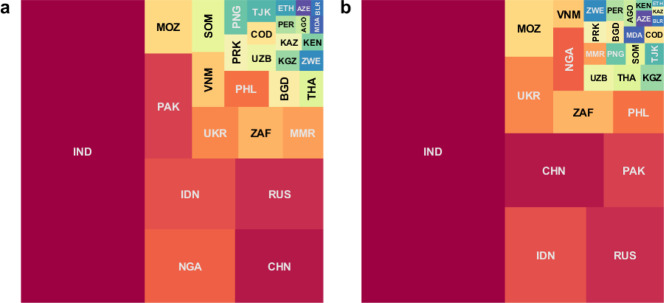
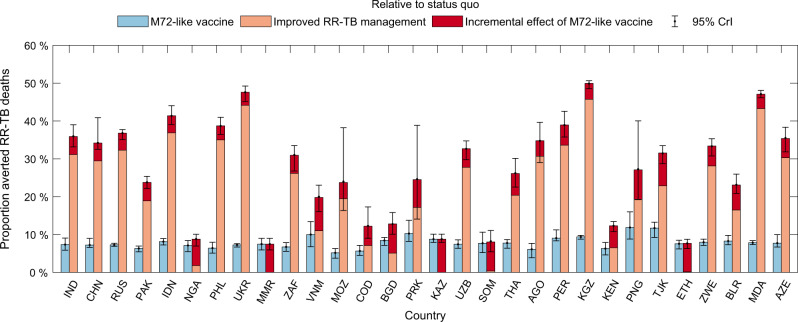
There have been notable advances in the development of vaccines against active tuberculosis (TB) disease for adults and adolescents. Using mathematical models, we seek to estimate the potential impact of a post-exposure TB vaccine, having 50% efficacy in reducing active disease, on global rifampicin-resistant (RR-) TB burden. In 30 countries that together accounted for 90% of global RR-TB incidence in 2018, a future TB vaccine could avert 10% (95% credible interval: 9.7-11%) of RR-TB cases and 7.3% (6.6-8.1%) of deaths over 2020-2035, with India, China, Indonesia, Pakistan, and the Russian Federation having the greatest contribution. This impact would increase to 14% (12-16%) and 31% (29-33%) respectively, when combined with improvements in RR-TB diagnosis and treatment relative to a scenario of no vaccine and no such improvements. A future TB vaccine could have important implications for the global control of RR-TB, especially if implemented alongside enhancements in management of drug resistance.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- World Health Organization. Global tuberculosis report 2019. https://apps.who.int/iris/bitstream/handle/10665/329368/9789241565714-en... (2019).
-
- World Health Organization. WHO consolidated guidelines on drug-resistant tuberculosis treatment. https://apps.who.int/iris/bitstream/handle/10665/311389/9789241550529-en... (2019). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
