

Exclusion of bacterial co-infection in COVID-19 using baseline inflammatory markers and their response to antibiotics
- PMID: 33463683
- PMCID: PMC7928909
- DOI: 10.1093/jac/dkaa563
Exclusion of bacterial co-infection in COVID-19 using baseline inflammatory markers and their response to antibiotics
Abstract
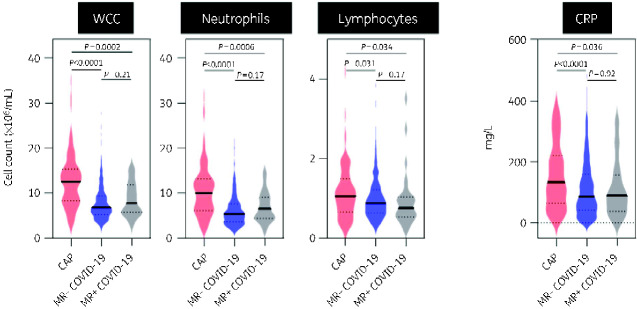
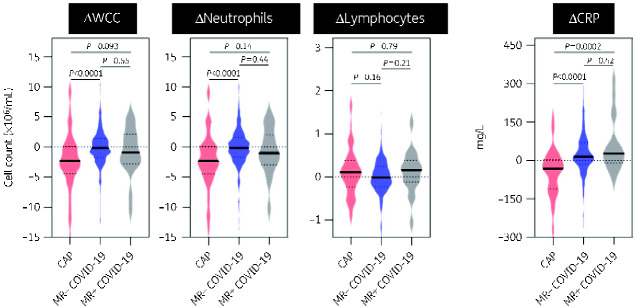
Background: COVID-19 is infrequently complicated by bacterial co-infection, but antibiotic prescriptions are common. We used community-acquired pneumonia (CAP) as a benchmark to define the processes that occur in bacterial pulmonary infections, testing the hypothesis that baseline inflammatory markers and their response to antibiotic therapy could distinguish bacterial co-infection from COVID-19.
Methods: Retrospective cohort study of CAP (lobar consolidation on chest radiograph) and COVID-19 (PCR detection of SARS-CoV-2) patients admitted to Royal Free Hospital (RFH) and Barnet Hospital (BH), serving as independent discovery and validation cohorts. All CAP and >90% COVID-19 patients received antibiotics on hospital admission.
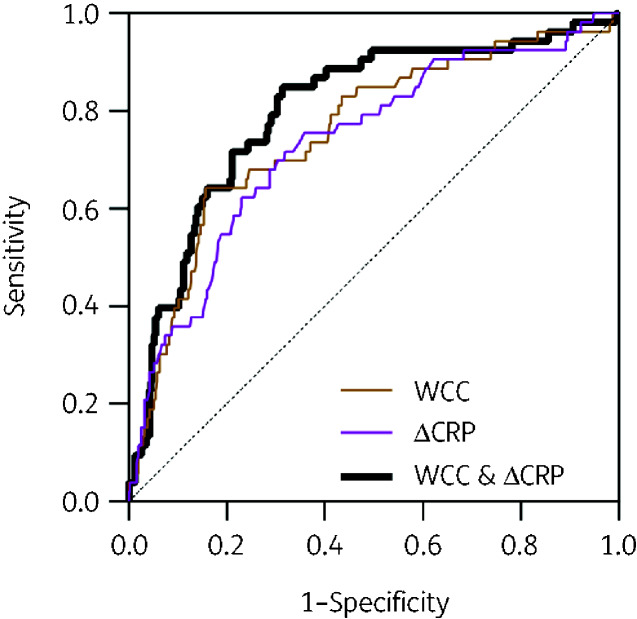
Results: We identified 106 CAP and 619 COVID-19 patients at RFH. Compared with COVID-19, CAP was characterized by elevated baseline white cell count (WCC) [median 12.48 (IQR 8.2-15.3) versus 6.78 (IQR 5.2-9.5) ×106 cells/mL, P < 0.0001], C-reactive protein (CRP) [median 133.5 (IQR 65-221) versus 86.0 (IQR 42-160) mg/L, P < 0.0001], and greater reduction in CRP 48-72 h into admission [median ΔCRP -33 (IQR -112 to +3.5) versus +14 (IQR -15.5 to +70.5) mg/L, P < 0.0001]. These observations were recapitulated in the independent validation cohort at BH (169 CAP and 181 COVID-19 patients). A multivariate logistic regression model incorporating WCC and ΔCRP discriminated CAP from COVID-19 with AUC 0.88 (95% CI 0.83-0.94). Baseline WCC >8.2 × 106 cells/mL or falling CRP identified 94% of CAP cases, and excluded bacterial co-infection in 46% of COVID-19 patients.
Conclusions: We propose that in COVID-19, absence of both elevated baseline WCC and antibiotic-related decrease in CRP can exclude bacterial co-infection and facilitate antibiotic stewardship efforts.
© The Author(s) 2021. Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- European Centre for Disease Prevention and Control. COVID-19 pandemic: situation update. https://www.ecdc.europa.eu/en/covid-19-pandemic.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
