

Stress hyperglycemia, cardiac glucotoxicity, and critically ill patient outcomes current clinical and pathophysiological evidence
- PMID: 33463901
- PMCID: PMC7814494
- DOI: 10.14814/phy2.14713
Stress hyperglycemia, cardiac glucotoxicity, and critically ill patient outcomes current clinical and pathophysiological evidence
Abstract
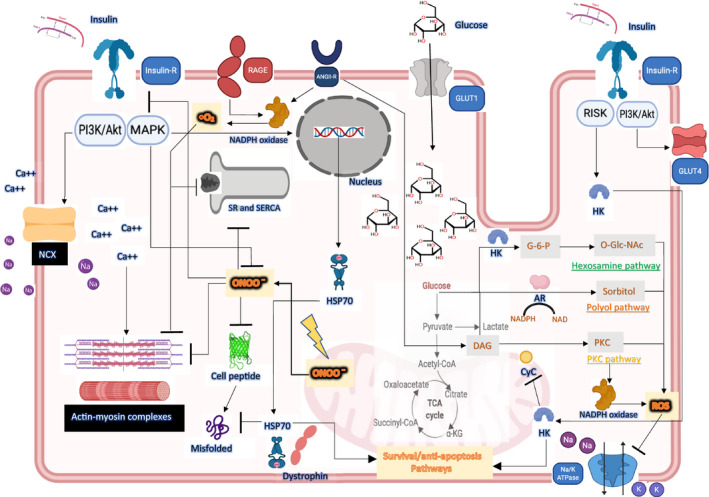
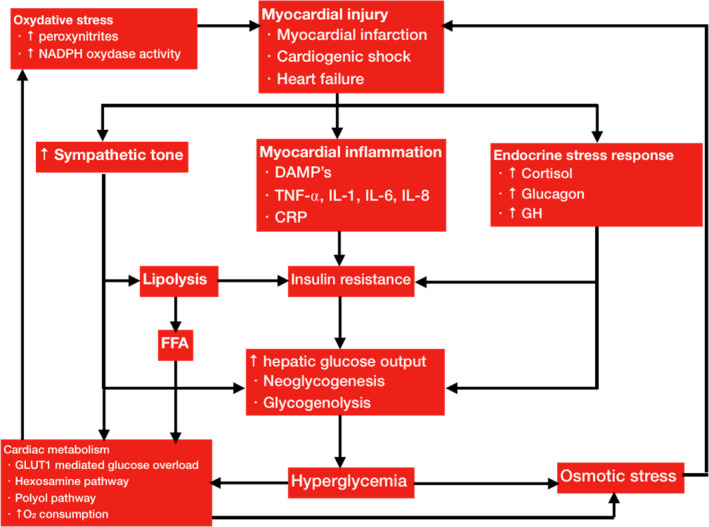
Stress hyperglycemia is a transient increase in blood glucose during acute physiological stress in the absence of glucose homeostasis dysfunction. Its's presence has been described in critically ill patients who are subject to many physiological insults. In this regard, hyperglycemia and impaired glucose tolerance are also frequent in patients who are admitted to the intensive care unit for heart failure and cardiogenic shock. The hyperglycemia observed at the beginning of these cardiac disorders appears to be related to a variety of stress mechanisms. The release of major stress and steroid hormones, catecholamine overload, and glucagon all participate in generating a state of insulin resistance with increased hepatic glucose output and glycogen breakdown. In fact, the observed pathophysiological response, which appears to regulate a stress situation, is harmful because it induces mitochondrial impairment, oxidative stress-related injury to cells, endothelial damage, and dysfunction of several cellular channels. Paradigms are now being challenged by growing evidence of a phenomenon called glucotoxicity, providing an explanation for the benefits of lowering glucose levels with insulin therapy in these patients. In the present review, the authors present the data published on cardiac glucotoxicity and discuss the benefits of lowering plasma glucose to improve heart function and to positively affect the course of critical illness.
Keywords: cardiogenic shock; glucotoxicity; heart; heart failure; insulin; stress hyperglycemia.
© 2021 The Authors. Physiological Reports published by Wiley Periodicals LLC on behalf of The Physiological Society and the American Physiological Society.
Conflict of interest statement
No conflicts of interest to declare.
Figures
Similar articles
-
[Glycaemia control in critically ill patients is justified and effective].Vnitr Lek. 2010 Sep;56(9 Suppl):977-87. Vnitr Lek. 2010. PMID: 21137171 Review. Czech.
-
Glucose control in the intensive care unit.Crit Care Med. 2009 May;37(5):1769-76. doi: 10.1097/CCM.0b013e3181a19ceb. Crit Care Med. 2009. PMID: 19325461 Review.
-
Feeding the critically ill obese patient: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Oct;13(10):95-109. doi: 10.11124/jbisrir-2015-2458. JBI Database System Rev Implement Rep. 2015. PMID: 26571286
-
Exogenous glucose administration impairs glucose tolerance and pancreatic insulin secretion during acute sepsis in non-diabetic mice.PLoS One. 2013 Jun 24;8(6):e67716. doi: 10.1371/journal.pone.0067716. Print 2013. PLoS One. 2013. PMID: 23826335 Free PMC article.
-
[Sepsis hyperglycemia in the ICU: from the mechanism to the clinic].Rev Med Chil. 2018 Apr;146(4):502-510. doi: 10.4067/s0034-98872018000400502. Rev Med Chil. 2018. PMID: 29999126 Review. Spanish.
Cited by
-
Weight loss, glycolipid profile changes in type 2 diabetes patients after esophagectomy: a propensity score matching analysis.Surg Endosc. 2024 Jun;38(6):3405-3415. doi: 10.1007/s00464-024-10852-5. Epub 2024 May 9. Surg Endosc. 2024. PMID: 38724646 Free PMC article.
-
Stress hyperglycemia ratio and the clinical outcome of patients with heart failure: a meta-analysis.Front Endocrinol (Lausanne). 2024 Jul 5;15:1404028. doi: 10.3389/fendo.2024.1404028. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39036054 Free PMC article.
-
Clinical Presentations and Predictors of In-Hospital Mortality in Illicit Drug Users in the New Psychoactive Substances (NPS) Endemic Era in Taiwan.Toxics. 2022 Jul 12;10(7):386. doi: 10.3390/toxics10070386. Toxics. 2022. PMID: 35878292 Free PMC article.
-
Mild Hyperglycaemia in Hospitalised Children with Moderate COVID-19 Infection.Medicina (Kaunas). 2023 May 14;59(5):944. doi: 10.3390/medicina59050944. Medicina (Kaunas). 2023. PMID: 37241176 Free PMC article.
-
Association between short-term systemic use of glucocorticoids and prognosis of cardiogenic shock: a retrospective analysis.BMC Anesthesiol. 2023 May 18;23(1):169. doi: 10.1186/s12871-023-02131-y. BMC Anesthesiol. 2023. PMID: 37202727 Free PMC article.
References
-
- Abdin, A. , Pöss, J. , Fuernau, G. , Ouarrak, T. , Desch, S. , Eitel, I. , de Waha, S. , Zeymer, U. , Böhm, M. , & Thiele, H. (2018). Revision: Prognostic impact of baseline glucose levels in acute myocardial infarction complicated by cardiogenic shock—A substudy of the IABP‐SHOCK II‐Trial. Clinical Research in Cardiology, 107, 517–523. - PubMed
-
- Abel, E. D. (2004). Glucose transport in the heart. Frontiers in Bioscience, 9, 201. - PubMed
-
- Aljada, A. , & Dandona, P. (2000). Effect of insulin on human aortic endothelial nitric oxide synthase. Metabolism, 49, 147–150. - PubMed
-
- Anand, I. S. , Latini, R. , Florea, V. G. , Kuskowski, M. A. , Rector, T. , Masson, S. , Signorini, S. , Mocarelli, P. , Hester, A. , Glazer, R. , & Cohn, J. N. (2005). C‐reactive protein in heart failure: Prognostic value and the effect of valsartan. Circulation, 112, 1428–1434. - PubMed
-
- Anker, S. D. , & Coats, A. J. (2002). How to recover from renaissance? The significance of the results of recover, renaissance, renewal and attach. International Journal of Cardiology, 86, 123–130. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
