

Association of the Intensity of Diagnostic Evaluation With Outcomes in Incidentally Detected Lung Nodules
- PMID: 33464296
- PMCID: PMC7816118
- DOI: 10.1001/jamainternmed.2020.8250
Association of the Intensity of Diagnostic Evaluation With Outcomes in Incidentally Detected Lung Nodules
Abstract
Importance: Whether guideline-concordant lung nodule evaluations lead to better outcomes remains unknown.
Objective: To examine the association between the intensity of lung nodule diagnostic evaluations and outcomes, safety, and health expenditures.
Design, setting, and participants: This comparative effectiveness research study analyzed health plan enrollees at Kaiser Permanente Washington in Seattle, Washington, and Marshfield Clinic in Marshfield, Wisconsin, with an incidental lung nodule detected between January 1, 2005, and December 31, 2015. Included patients were 35 years or older, had no high suspicion of infection, had no history of malignant neoplasm, and had no evidence of advanced lung cancer on nodule detection. Data analysis was conducted from January 7 to August 19, 2020.
Exposures: With the 2005 Fleischner Society guidelines (selected for their applicability to the time frame under investigation) as the comparator, 2 other intensities of lung nodule evaluation were defined. Guideline-concordant evaluation followed the guidelines. Less intensive evaluation was the absence of recommended testing, longer-than-recommended surveillance intervals, or less invasive testing than recommended. More intensive evaluation consisted of testing when the guidelines recommended no further testing, shorter-than-recommended surveillance intervals, or more invasive testing than recommended.
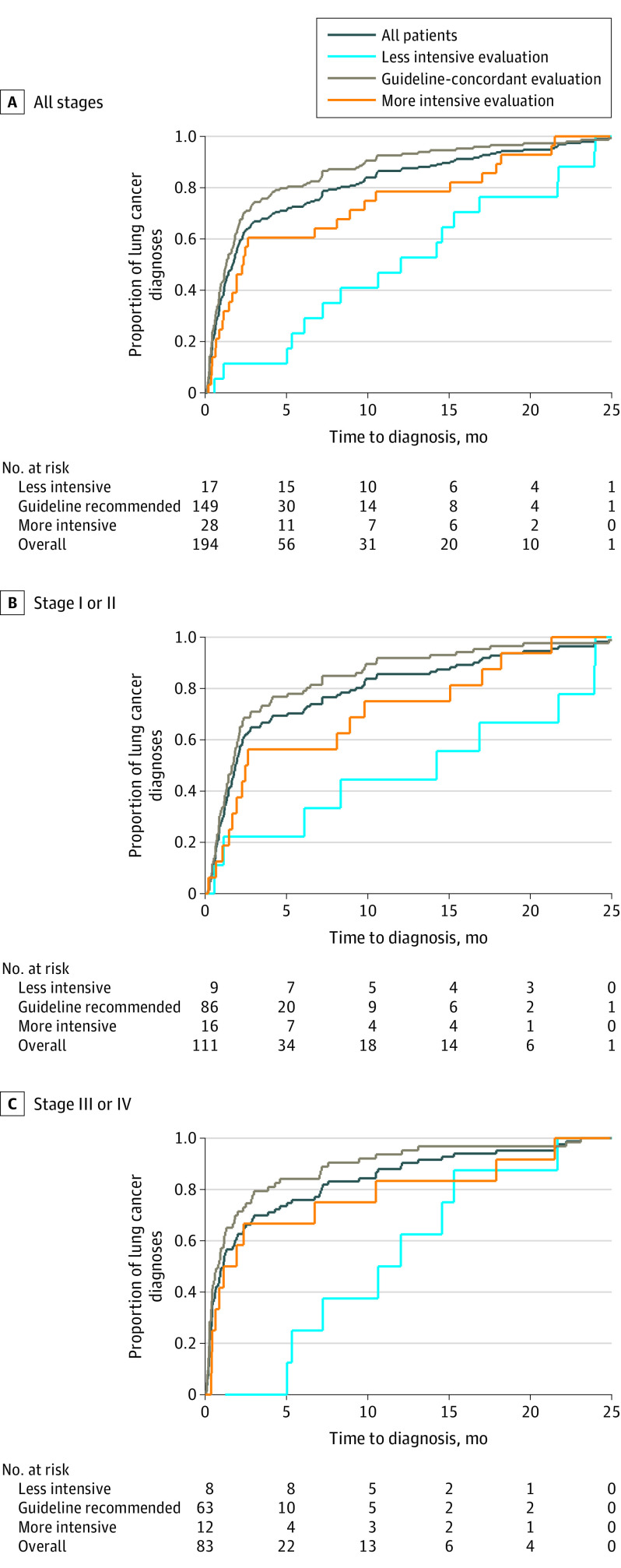
Main outcomes and measures: The main outcome was the proportion of patients with lung cancer who had stage III or IV disease, radiation exposure, procedure-related adverse events, and health expenditures 2 years after nodule detection.
Results: Among the 5057 individuals included in this comparative effectiveness research study, 1925 (38%) received guideline-concordant, 1863 (37%) less intensive, and 1269 (25%) more intensive diagnostic evaluations. The entire cohort comprised 2786 female patients (55%), and the mean (SD) age was 67 (13) years. Adjusted analyses showed that compared with guideline-concordant evaluations, less intensive evaluations were associated with fewer procedure-related adverse events (risk difference [RD], -5.9%; 95% CI, -7.2% to -4.6%), lower mean radiation exposure (-9.5 milliSieverts [mSv]; 95% CI, -10.3 mSv to -8.7 mSv), and lower mean health expenditures (-$10 916; 95% CI, -$16 112 to -$5719); no difference in stage III or IV disease was found among patients diagnosed with lung cancer (RD, 4.6%; 95% CI, -22% to +31%). More intensive evaluations were associated with more procedure-related adverse events (RD, +8.1%; 95% CI, +5.6% to +11%), higher mean radiation exposure (+6.8 mSv; 95% CI, +5.8 mSv to +7.8 mSv), and higher mean health expenditures ($20 132; 95% CI, +$14 398 to +$25 868); no difference in stage III or IV disease was observed (RD, -0.5%; 95% CI, -28% to +27%).
Conclusions and relevance: This study found inconclusive evidence of an association between less intensive diagnostic evaluations and more advanced stage at lung cancer diagnosis compared with guideline-concordant care; higher intensities of diagnostic evaluations were associated with greater procedural complications, radiation exposure, and expenditures. These findings underscore the need for more evidence on better ways to evaluate lung nodules and to avoid unnecessarily intensive diagnostic evaluations of lung nodules.
Conflict of interest statement
Figures
Comment in
-
Beyond the AJR: "Association of the Intensity of Diagnostic Evaluation With Outcomes in Incidentally Detected Lung Nodules".AJR Am J Roentgenol. 2021 Oct;217(4):1011. doi: 10.2214/AJR.21.25903. Epub 2021 Mar 31. AJR Am J Roentgenol. 2021. PMID: 33787287 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
